CASE20230819_003
Severely Calcification-Induced Ruptured Lithotripsy Balloon in ECMO-Assisted CHIP-PCI
By Hsin-I Teng
Presenter
Hsin-I Teng
Authors
Hsin-I Teng1
Affiliation
CHGH, Taiwan1,
View Study Report
CASE20230819_003
Complex PCI - Calcified Lesion
Severely Calcification-Induced Ruptured Lithotripsy Balloon in ECMO-Assisted CHIP-PCI
Hsin-I Teng1
CHGH, Taiwan1,
Clinical Information
Relevant Clinical History and Physical Exam
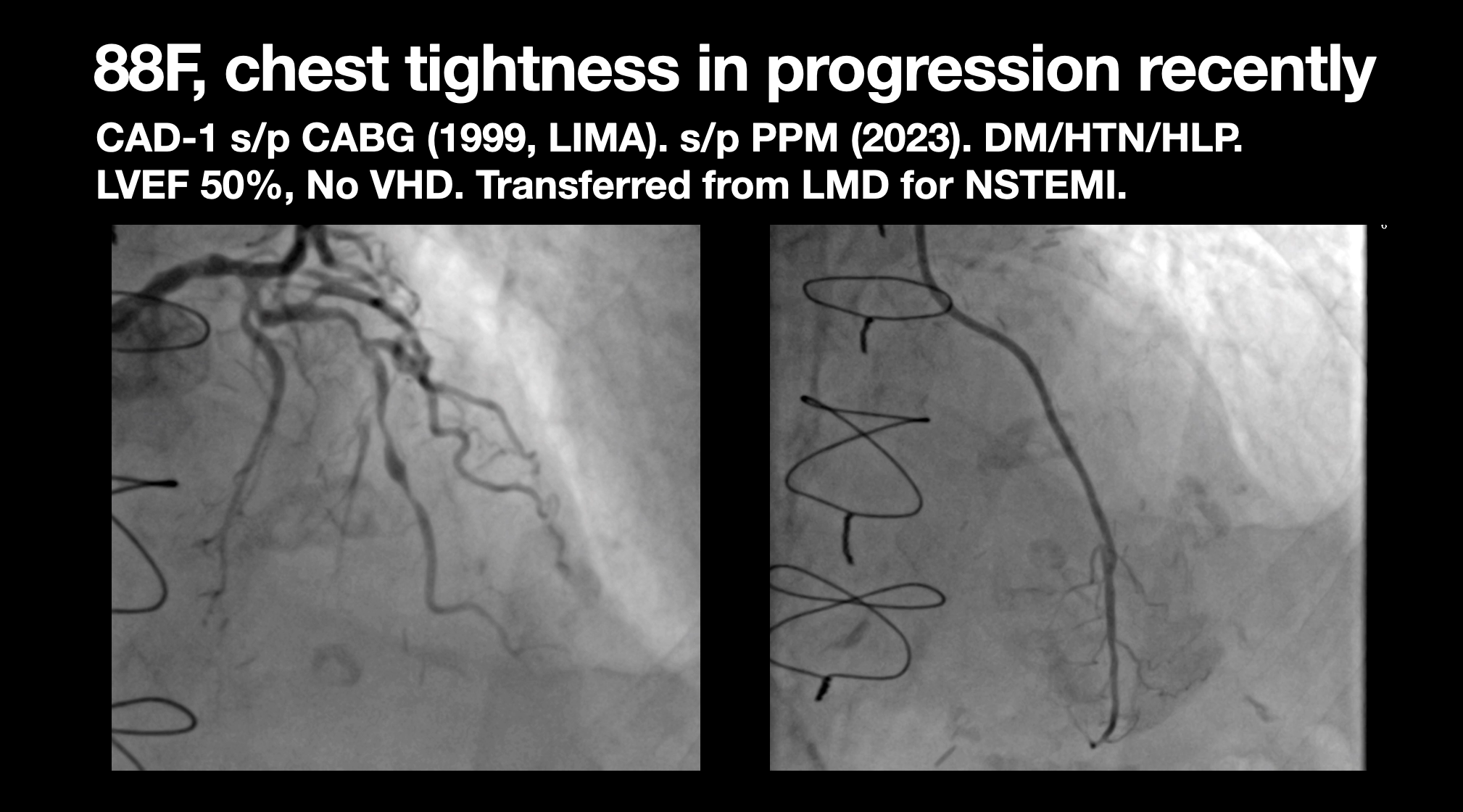
This 88y woman had chest pain in progression recently. She had diabetes, hypertension, hyperlipidemia and one vessel disease status post CABG in 1999 with LIMA. Besides, she also had PPM in 2023. Her LVEF 50%. This time, she was referred from local hospital for IVL and Rota.
Relevant Test Results Prior to Catheterization
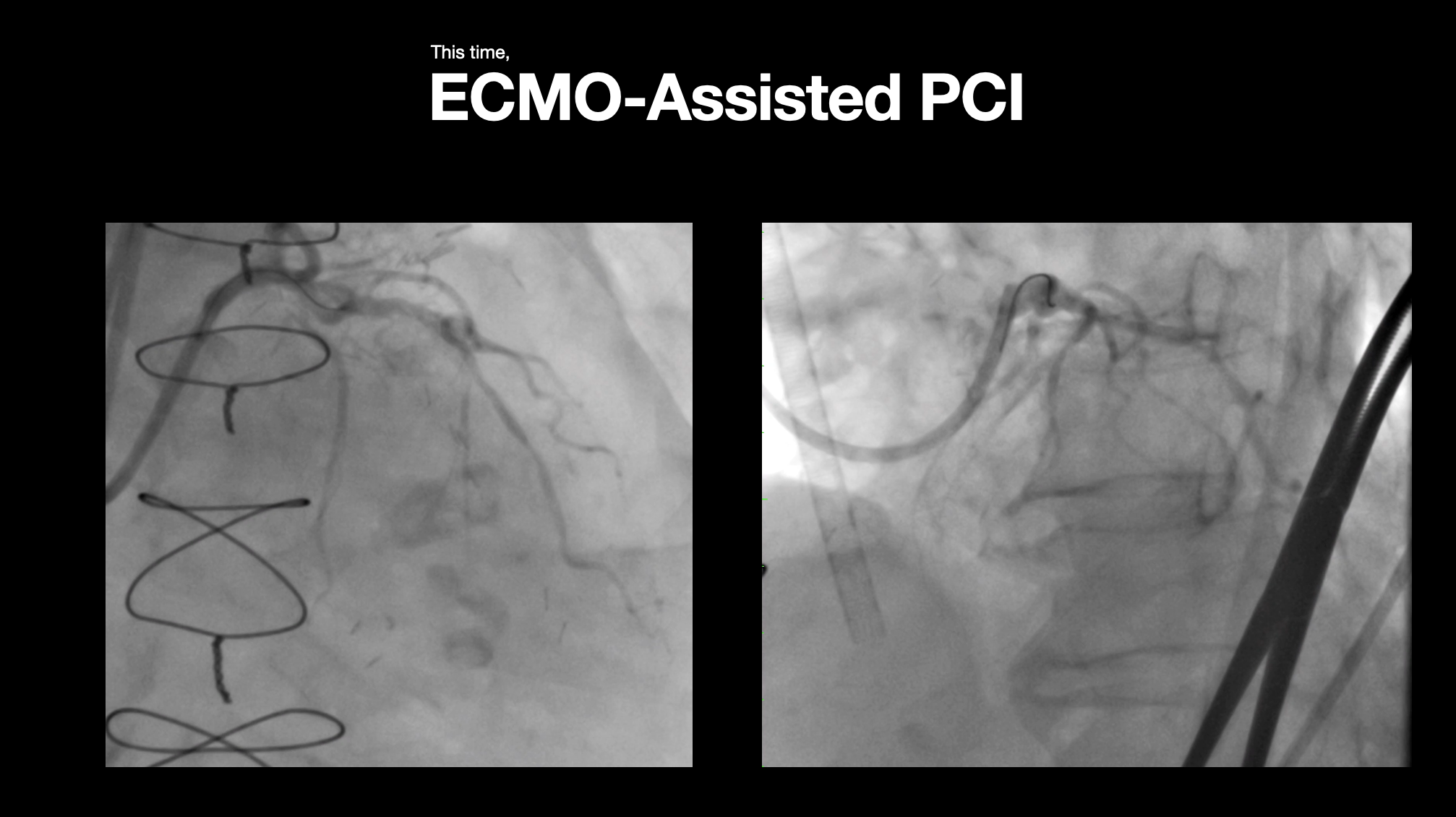
Sudden collapse was noted at ward while walking around with walker. ECMO-assisted PCI was initiated.
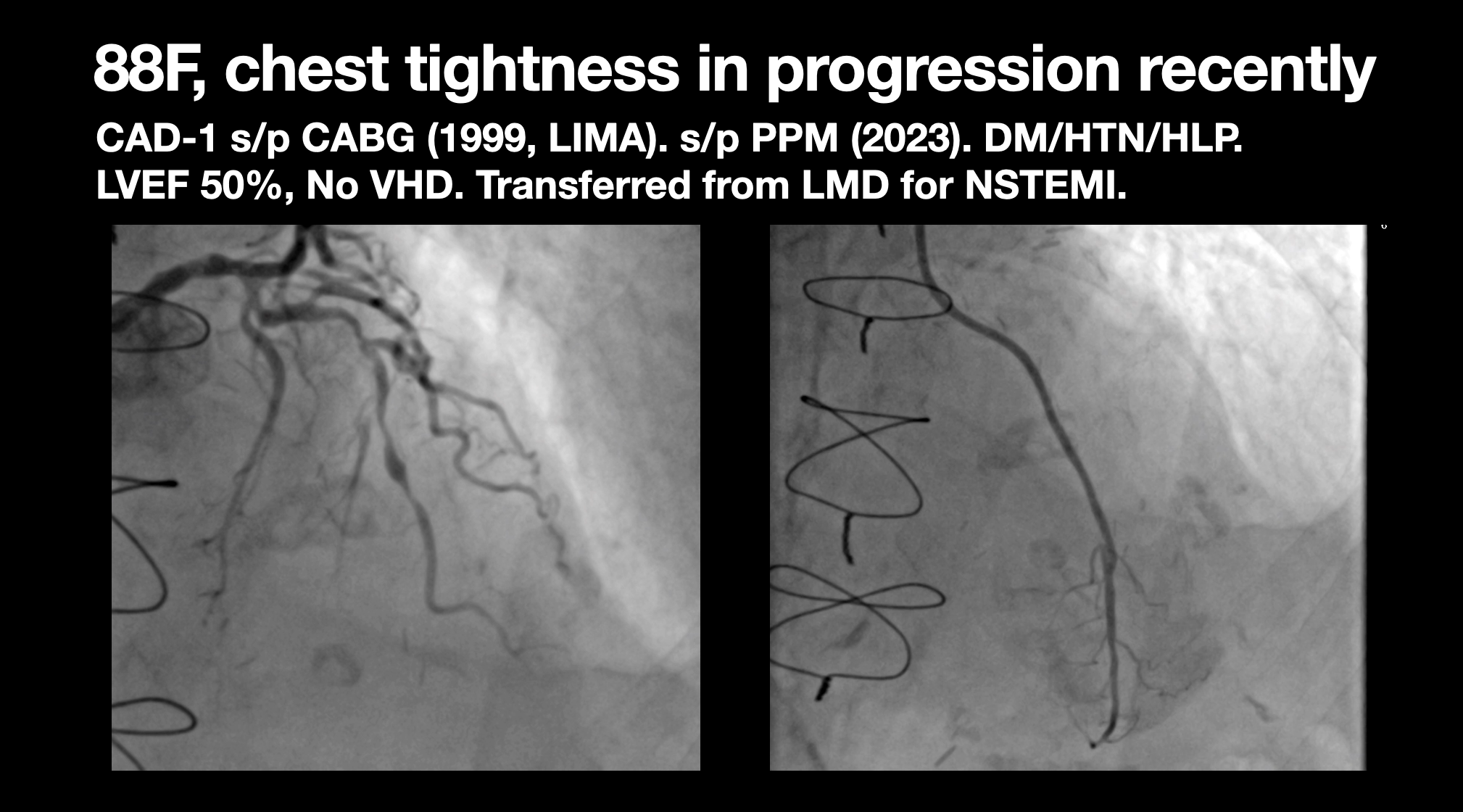
Relevant Catheterization Findings
Because sudden collapse followed by ECMO-assisted PCI was initiated. CAG showed severe LM calcified nodules and LAD long diffuse and severe eccentric calcium. IVUS confirmed this findings. NC BC followed by IVL NC ruptured was noted while inflation. IVUS check showed BC skin was attached at LM bifurcation. We used different techniques and tried to rescue the ruptured BC but in vain. Finally, under IVUS guidance, we succeed in putting stent in LM bifurcation LAD without LCX jailing.

Interventional Management
Procedural Step
We advanced NC BC to pass the severely calcified lesion but rupture. Due to slow flow after BC rupture, further rota was not considered. Then we advanced one IVL BC. However, IVL BC ruptured again. Then we tried anchor technique with BC and extension catheter but in vain. IVUS check showed the BC skin was busted located at bifurcation site. But by the guidance of IVUS. finally we can put a stent to compress the BC skin and successfully avoid LCX jailing while stenting. Finally, ECMO was removed after PCI and the patient recovered well with regular OPD follow up.
Case Summary
What I learned in this case are as below. Firstly, elderly patient exhibited remarkable frailty and have restricted tolerance. Secondly, mechanical support is crucial in CHIP-PCI. Thirdly, Half-way rota to facilitate IVL delivery might be an option in this tortuous and severely calcified LAD vessel. Finally, trying our best to optimize the results with imaging guidance is really importance to get good longterm results.