CASE20230821_004
A Case of Transcatheter Coil Embolization for Pulmonary Arteriovenous Malformation Complicated With Transient St Elevation, Heart Block and Hypotension
By Lok Hang Canice Ng, Chris Kwok Yiu Wong, Wai Chee Walter Chen
Presenter
Lok Hang Canice Ng
Authors
Lok Hang Canice Ng1, Chris Kwok Yiu Wong, Wai Chee Walter Chen1
Affiliation
The Heart Clinic, Hong Kong, China1,
View Study Report
CASE20230821_004
Adjuctive Procedures - Adjuctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
A Case of Transcatheter Coil Embolization for Pulmonary Arteriovenous Malformation Complicated With Transient St Elevation, Heart Block and Hypotension
Lok Hang Canice Ng1, Chris Kwok Yiu Wong, Wai Chee Walter Chen1
The Heart Clinic, Hong Kong, China1,
Clinical Information
Relevant Clinical History and Physical Exam
This was a 73 years old gentleman with history of anxiety, hypertension and diabetes mellitus complained of shortness of breath since 2017.Electrocardiogram showed sinus rhythm without any ST changes. Echocardiogram showed left ventricular diastolic dysfunction. Treadmill exercise test was normal.
Relevant Test Results Prior to Catheterization
CT angiogram showed no significant stenosis over coronary arteries but found pulmonary arteriovenous malformation. CT pulmonary angiogram repeated in 6/2023 showed a simple type pulmonary arteriovenous malformation sized around 4.7 x 7.1 x 3.8 cm, which was supplied by single segmental branch of right lower lobar pulmonary artery. As his symptoms persisted and his oxygen saturation was always below 92% properly due to the large shunt, patient agreed for pulmonary AVM embolization.

Relevant Catheterization Findings
His oxygen saturation on room air was often below 90% during pre-operation assessment. The procedure was done under monitored anesthesia case. Right femoral vein was punctured and 7 Fr shuttle sheath and 6 Fr multipurpose catheter were advanced to right pulmonary artery. The baseline pulmonary pressure and ECG were normal. Pulmonary angiogram was performed and the orifice of the AV fistula was identified.
 3. selective angiogram via mic cath .mov
3. selective angiogram via mic cath .mov

Interventional Management
Procedural Step
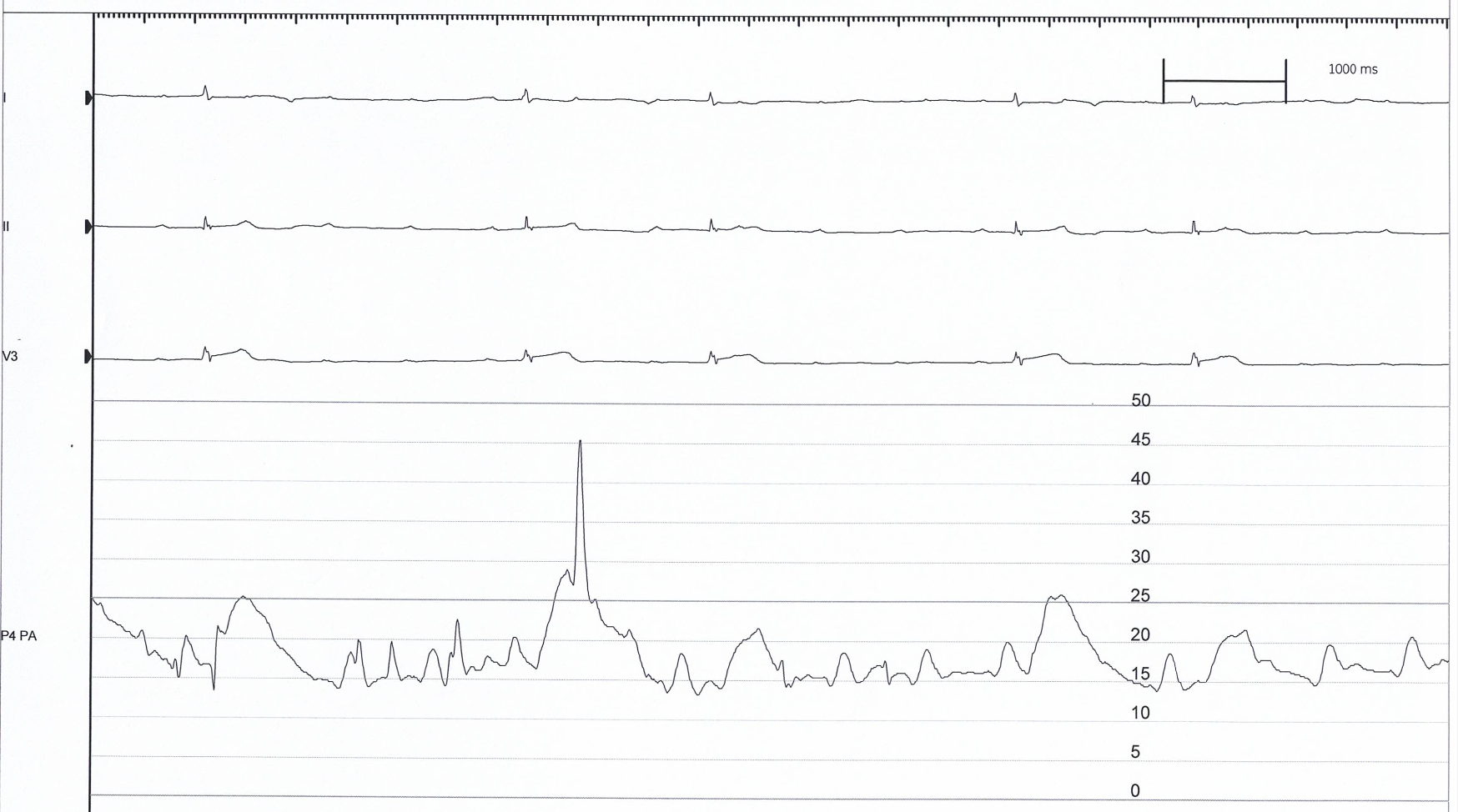
The procedure was done under monitored anesthesia case. Right femoral vein was punctured and 7 Fr shuttle sheath and 6 Fr multipurpose catheter were advanced to right pulmonary artery. The baseline pulmonary pressure and ECG were normal. Pulmonary angiogram was performed and the orifice of the AV fistula was identified. Excelsior 1018 microcatheter was then advanced into the AV fistula. Target coil (XXL 360) 24 x 50, 24 x 50 cm and 14 x 50 cm were deployed into the AV fistula. After embolization, there was a transient ST elevation over lead V3 and 2nd degree AV block, RBBB and hypotension. Dopamine infusion was given. Right and left coronary angiogram was performed and there was no significant stenosis. Bedside Echocardiogram showed normal LV and RV function and no pericardial effusion. After dopamine infusion, ST elevation and arrhythmia resolved and blood pressure returned to normal. Post-procedure pulmonary angiogram showed the AV fistula was totally blocked. Oxygen saturation was 94-95 %. Arterial puncture was closed with Angioseal. Venous puncture was closely by fisherman knot. Patient recovered well and discharged on next day. Patient was followed up 1 week after operation. He had less shortness of breath and his exercise tolerance was improved.
10. final 2.mov
5. 1st coil deploy.mp4
Case Summary
Current recommendations based on observational studies suggest that all PAVMs suitable for embolisation (regardless of size) should be treated, whereas the role of surgery may be limited in patients with PAVMs not suitable for embolisation. TThe rate of procedure complication is extremely low but rare serious complications such as air embolism may still occur. From the literature review, air embolism during embolisation was suspected in 4.8 % of patients. Small air emboli have a propensity to enter the coronary arteries during procedure causing acute chest pain, bradycardia, and temporary ECG changes. This usually resolves with sublingual nitroglycerin and inotrope support.