CASE20250603_001
Predicting Future Cardiovascular events by Lipid Core Burden index.(LCBI)
By Farrukh Malik
Presenter
Farrukh Malik
Authors
Farrukh Malik1
Affiliation
National Institute of Cardiovascular Diseases, Pakistan1
View Study Report
CASE20250603_001
Clinical Trials & Science - Clinical Trials & Science
Predicting Future Cardiovascular events by Lipid Core Burden index.(LCBI)
Farrukh Malik1
National Institute of Cardiovascular Diseases, Pakistan1
Clinical Information
Relevant Clinical History and Physical Exam
Vulnerable coronary plaques, particularly those rich in lipid content, are key contributors to the onset of acute coronary syndromes. The Lipid Core Burden Index (LCBI) has gained attention as a promising imaging biomarker for detecting patients who may be at increased risk of experiencing future major adverse cardiovascular events (MACE). Near-infrared spectroscopy (NIRS) is a imaging technique that detects plaques with high lipid content, which is a critical indicator of plaque vulneribilty
Relevant Test Results Prior to Catheterization
This study evaluates the prognostic utility of NIRS-derived LCBI in predicting MACE in patients undergoing coronary angiography.We conducted a prospective study at National Institute of Cardiovascular diseases involving 100 patients undergoing NIRS-IVUS imaging during clinically indicated coronary catheterization. The primary endpoint was a composite of MACE at 12 months. Non-culprit lesions were imaged using Makoto NIRS-IVUS, and the highest LCBI was recorded for each patient.
Relevant Catheterization Findings
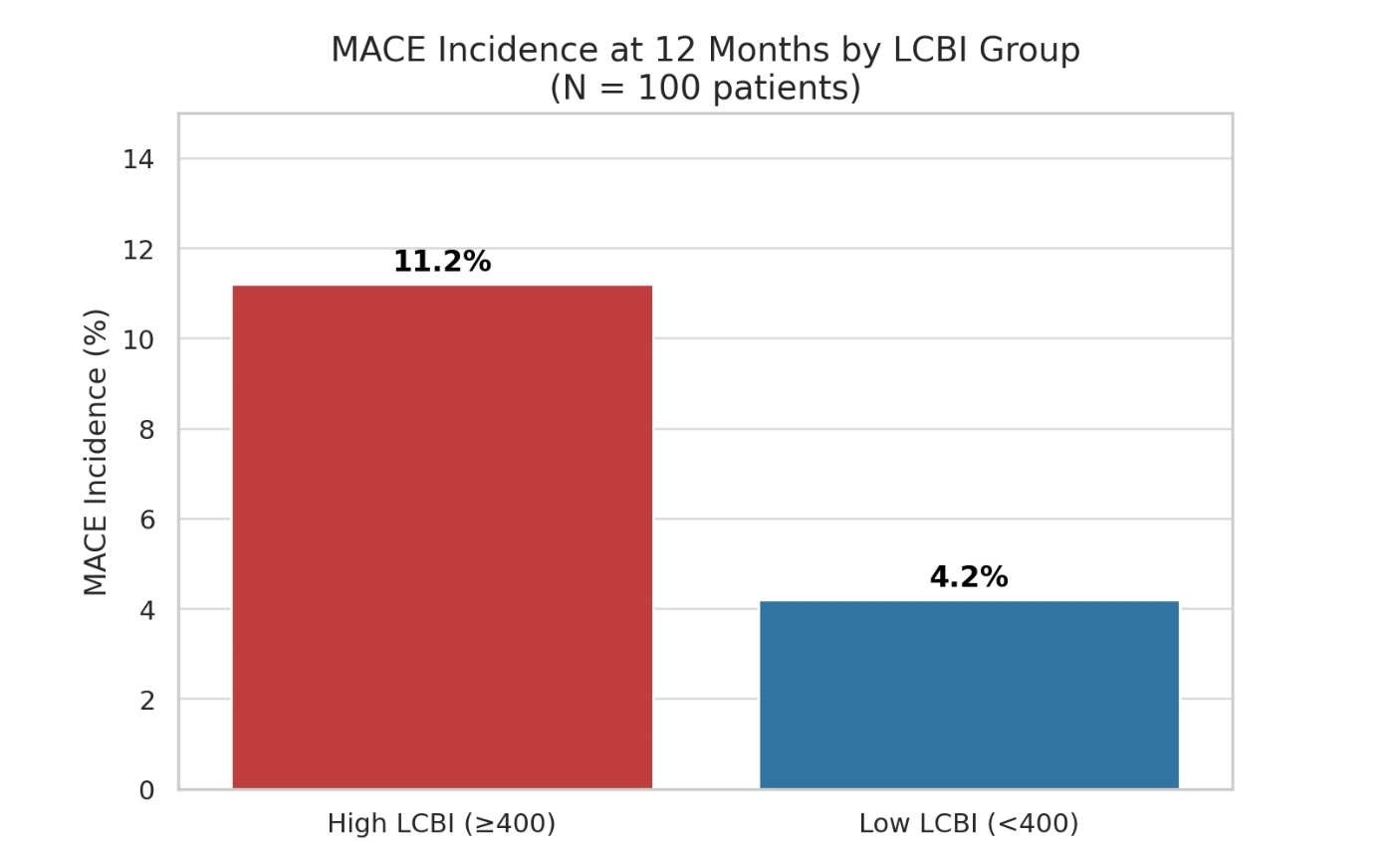
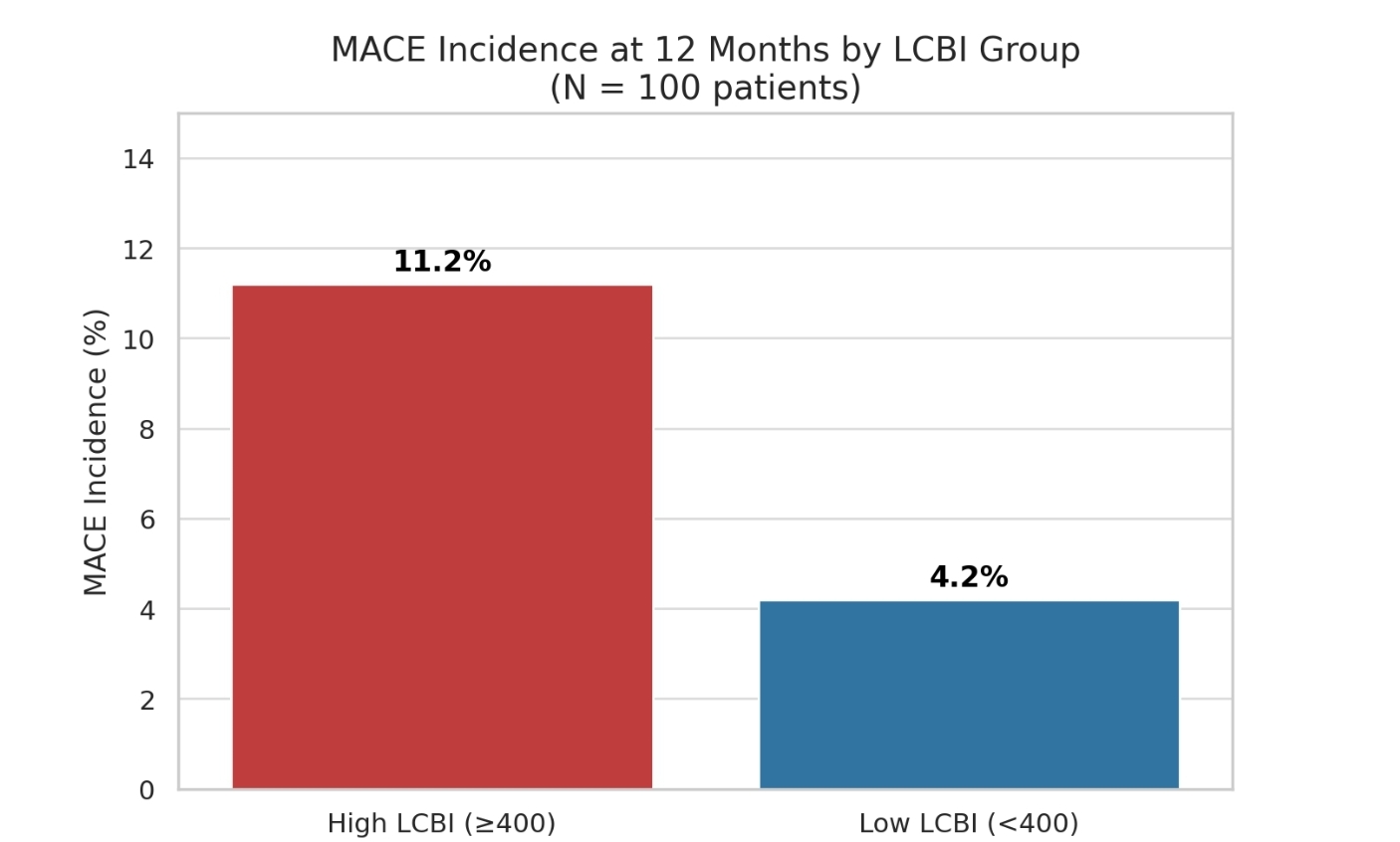
Patients were stratified into two groups based on LCBI values: high-risk (≥400) and low-risk (<400). Event rates were compared using Kaplan-Meier analysis, and Cox proportional hazards modeling was used to assess the independent predictive value of LCBI.Among 100 patients (mean age 64±9 years; 72% male), 23 % had a non-culprit lesion with LCBI ≥400. At 12 month follow-up, the incidence of MACE was significantly higher in the high-LCBI group compared to the low-LCBI group 11.2% vs. 4.2%,.
Interventional Management
Procedural Step
Among 100 patients (mean age 64±9 years; 72% male), 23 % had a non-culprit lesion with LCBI ≥400. At 12 month follow-up, the incidence of MACE was significantly higher in the high-LCBI group compared to the low-LCBI group (11.2% vs. 4.2%, p<0.001).After adjusting for traditional risk factors and angiographic stenosis severity, LCBI ≥400 remained an independent predictor of MACE (adjusted HR 3.6; 95% CI 2.1–6.2; p<0.001). Notably, most events occurred at sites with <70% angiographic stenosis, highlighting the added value of plaque characterization beyond lumen assessment.
Case Summary
Conclusion:NIRS-derived LCBI is a robust and independent predictor of future MACE in patients undergoing coronary angiography. An LCBI threshold of ≥400 identifies high-risk plaques in non-culprit segments, often missed by angiography alone. Incorporating NIRS imaging into routine clinical practice may enhance risk stratification and guide targeted preventive therapies in patients with coronary artery disease.