CASE20250604_001
Double Jeopardy in Time Crisis
By Wittawat Wattanasiriporn
Presenter
Wittawat Wattanasiriporn
Authors
Wittawat Wattanasiriporn1
Affiliation
Rajavithi Hospital, Thailand1
View Study Report
CASE20250604_001
Hemodynamic Support - Hemodynamic Support
Double Jeopardy in Time Crisis
Wittawat Wattanasiriporn1
Rajavithi Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
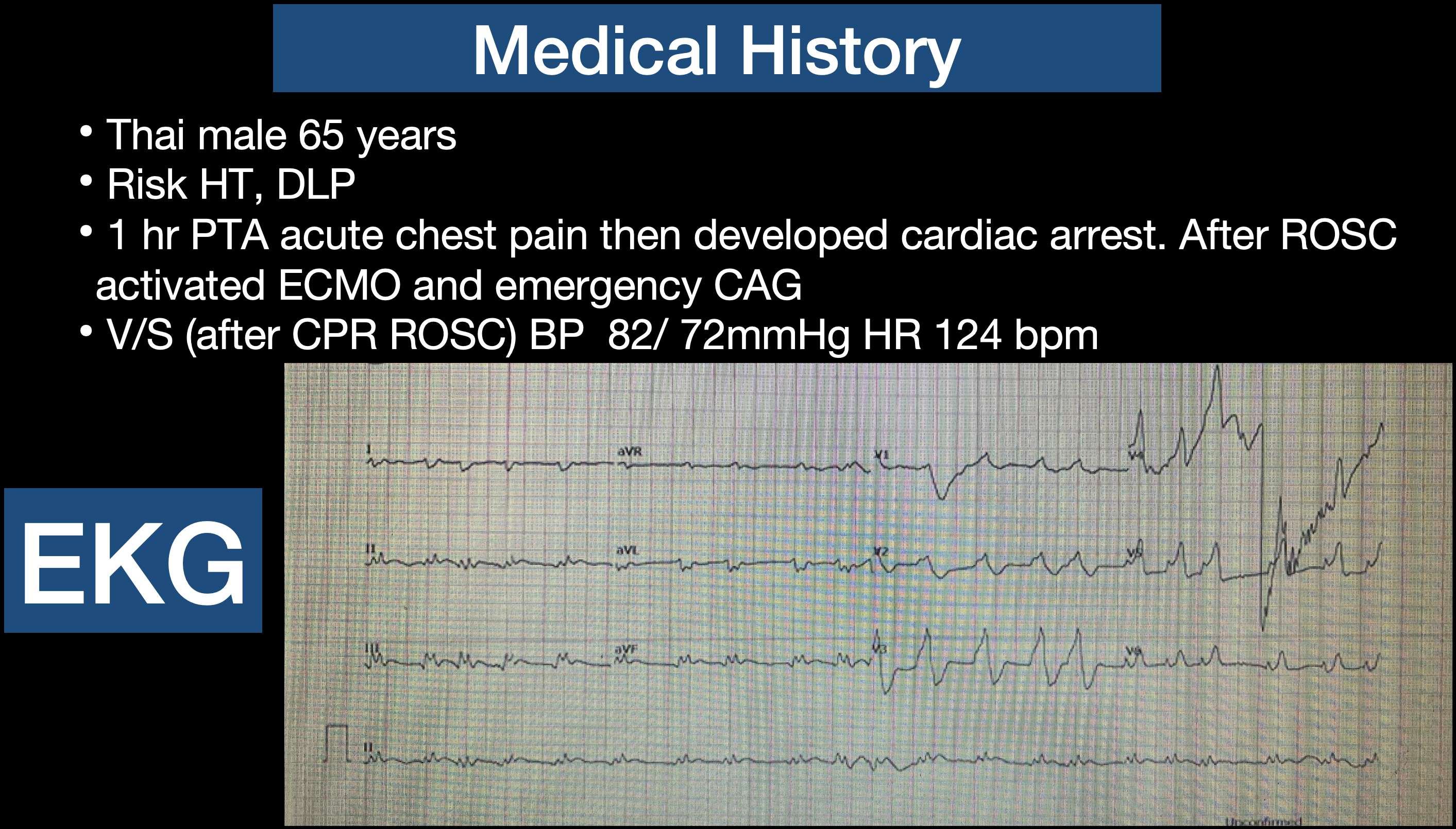
Thai male 65 years, Risk HT, DLP. Presented with 1 hr PTA acute chest pain then developed cardiac arrest. After ROSC activated ECMO and emergency CAG. After CPR ROSC, BP 82/ 72mmHg HR 124 bpm, heart totally regular, fine crepitation both lungs.
Relevant Test Results Prior to Catheterization
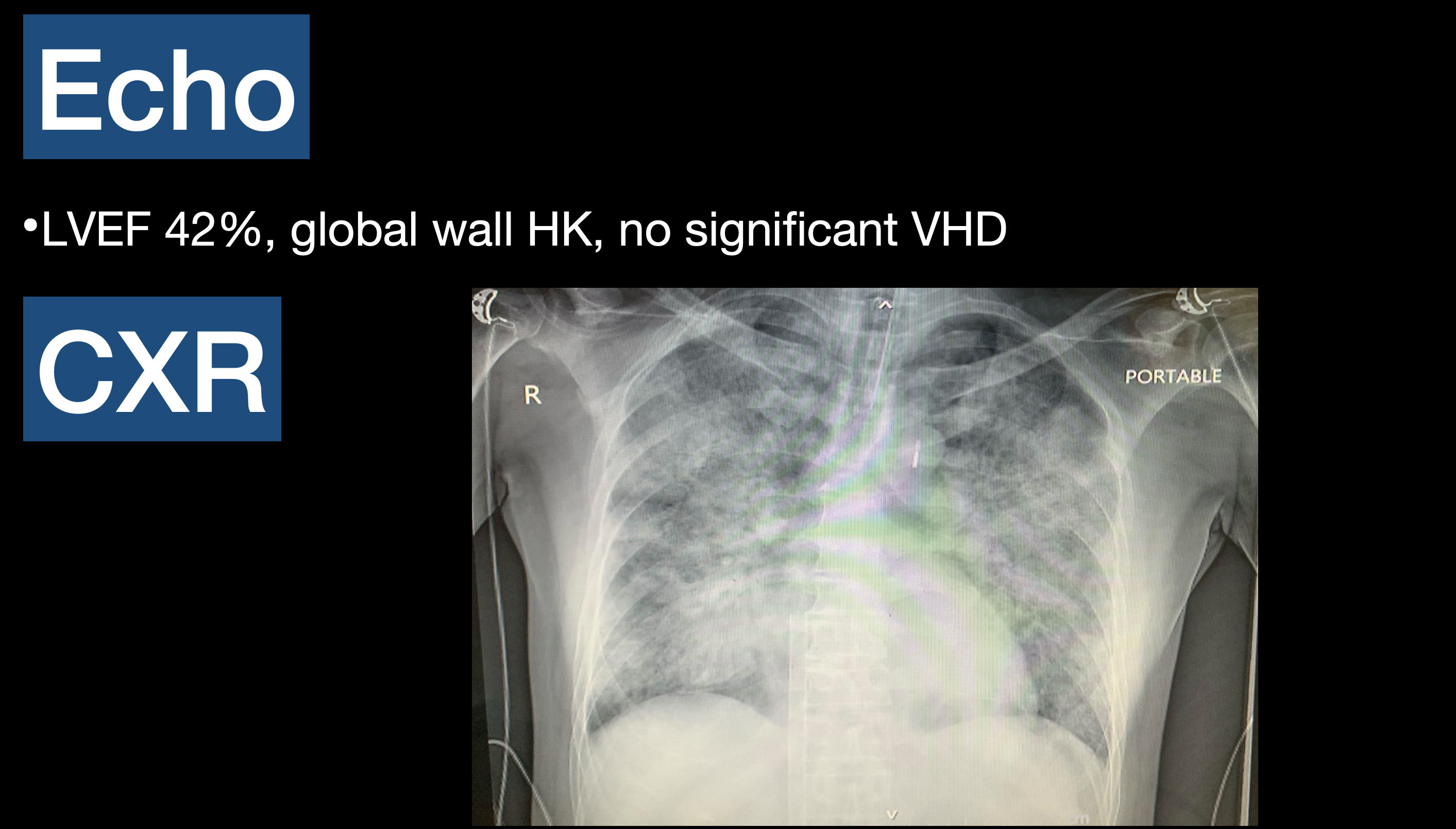
EKG showed AF with Rapid ventricular response 120 bpm, minimal ST elevation at II, III, aVF. Echocardiogram showed LVEF 42%, global wall HK, no significant VHD. Chest x ray showed mild cardiomegaly, bilateral pulmonary congestion.
Relevant Catheterization Findings
CAG via 7Fr RFA Sheath with Diagnostic catheter JL 4.0/6 Fr, JR 4.0/6Fr showed Rt dominant, LM: 30-40% stenosis distal LM, LAD: 80-90% stenosis proximal to mid LAD c filling defect, 70-80%stenosis DG1, LCx: subtotal occlusion small OM1, RCA: 20-30% stenosis proximal RCA, CTO mid RCA.

Interventional Management
Procedural Step
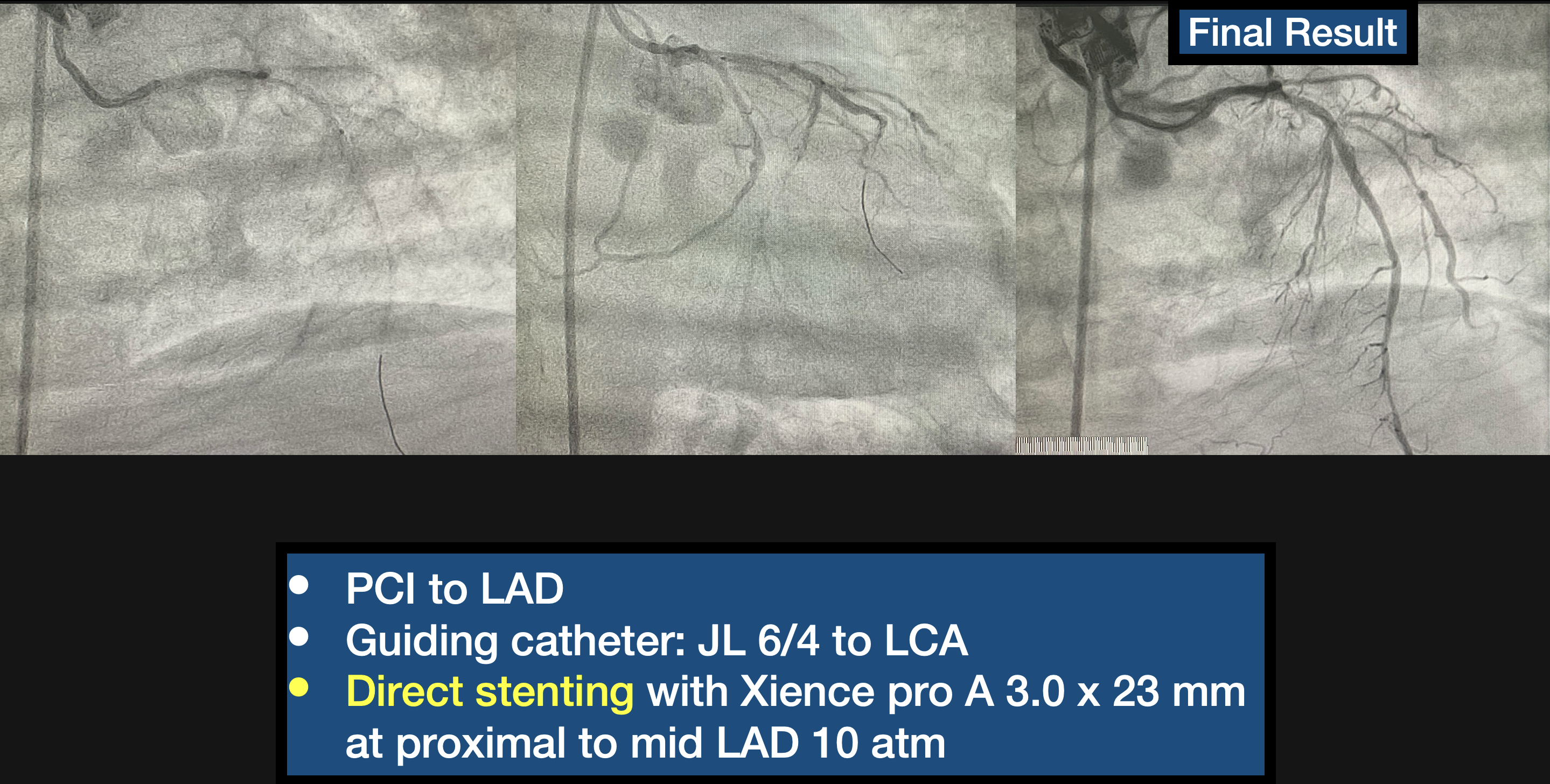
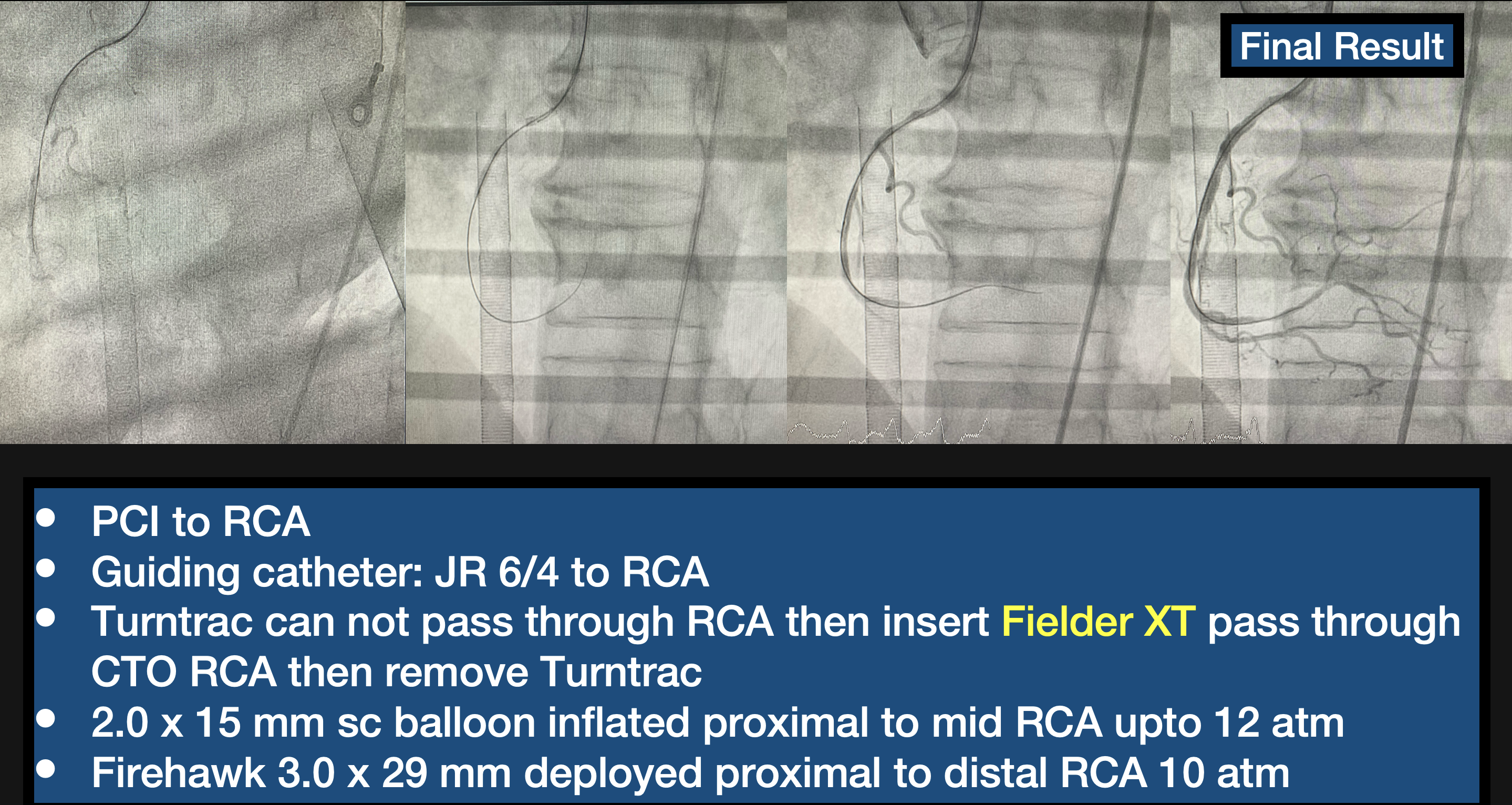
CAG via 7Fr RFA Sheath with Diagnostic catheter JL 4.0/6 Fr, JR 4.0/6Fr showed Rt dominant, LM: 30-40% stenosis distal LM, LAD: 80-90% stenosis proximal to mid LAD c filling defect, 70-80%stenosis DG1, LCx: subtotal occlusion small OM1, RCA: 20-30% stenosis proximal RCA, CTO mid RCA.PCI to LAD,Guiding catheter: JL 6/4 to LCA. Direct stenting with Xience pro A 3.0 x 23 mm at proximal to mid LAD 10 atm. PCI to RCA, Guiding catheter: JR 6/4 to RCA. Turntrac can not pass through RCA then insert Fielder XT pass through CTO RCA then remove Turntrac. 2.0 x 15 mm sc balloon inflated proximal to mid RCA upto 12 atm. Firehawk 3.0 x 29 mm deployed proximal to distal RCA 10 atm.
Case Summary
1.VA ECMO support during PCI is a safe and feasible strategy to achieve revascularization in complex and high risk patient