CASE20250706_001
Refuse to Give Up: Retrograde Approach Without Microcatheter
By Mahesh Shivaji Ahire, Gaurav Verma
Presenter
Mahesh Shivaji Ahire
Authors
Mahesh Shivaji Ahire1, Gaurav Verma1
Affiliation
SMBT Heart Institue, India1
View Study Report
CASE20250706_001
Complex PCI - CTO
Refuse to Give Up: Retrograde Approach Without Microcatheter
Mahesh Shivaji Ahire1, Gaurav Verma1
SMBT Heart Institue, India1
Clinical Information
Relevant Clinical History and Physical Exam
63 An old female patient presented with unstable angina for 6 months, k/c/o HTN, TYPE II DM, 2DECHO S/O LVEF 45% WITH INFERIOR WALL HYPOKINESIA WITH PRESERVED WALL THICKNESS., CAG S/O TVD WITH RCA CTO
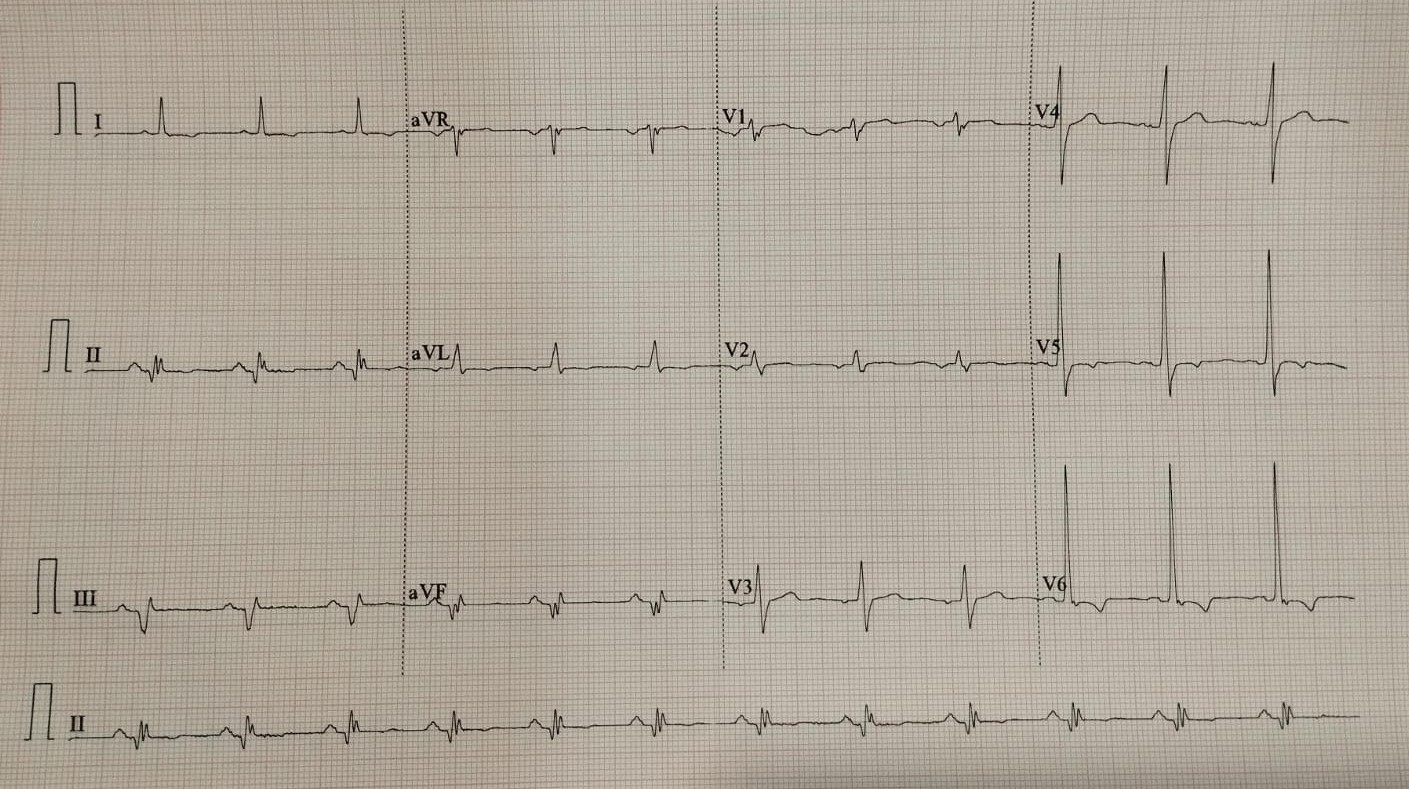
Relevant Test Results Prior to Catheterization
2D ECHO S/O INFERIOR WALL HYPOKINESIA , LVEF45% WITH PRESERVED WALL THICKNESS.
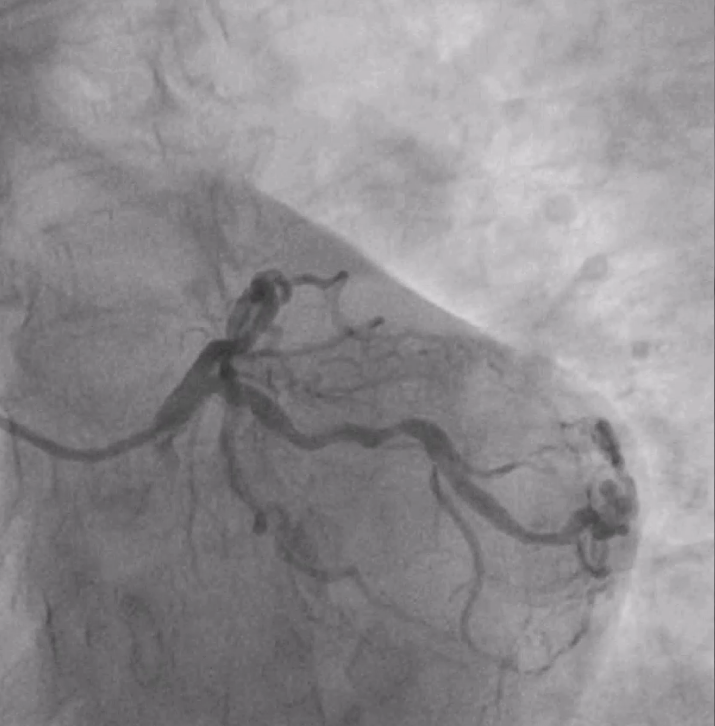
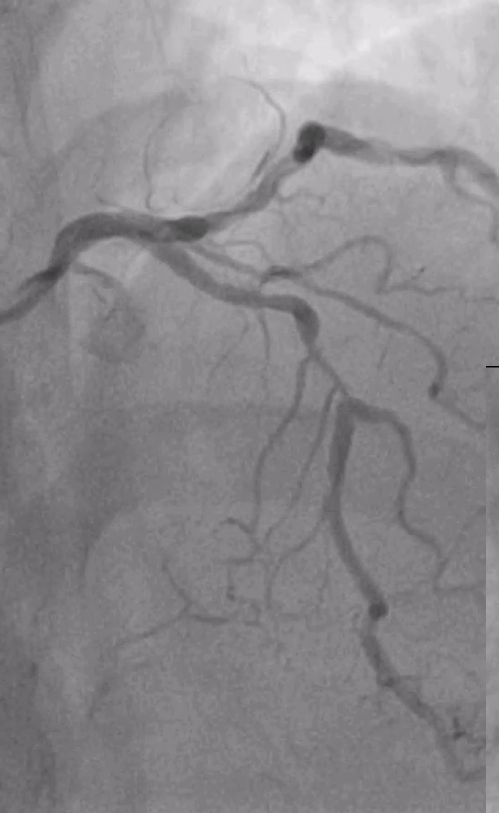
Relevant Catheterization Findings
CAG S/O TRIPLE VESSEL DISEASE, WITH RCA CTO FILLING RETROGATELY. ADVICE CABG BUT PATIENT IS NOT WILLING FOR CABG
Interventional Management
Procedural Step
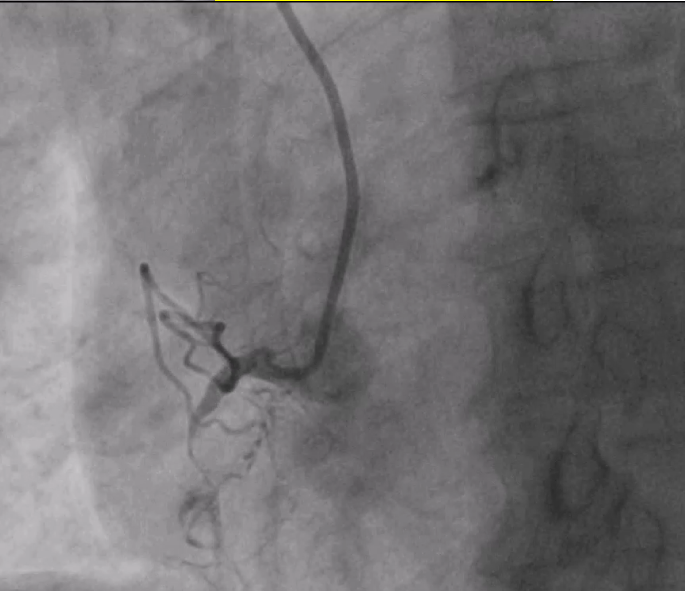
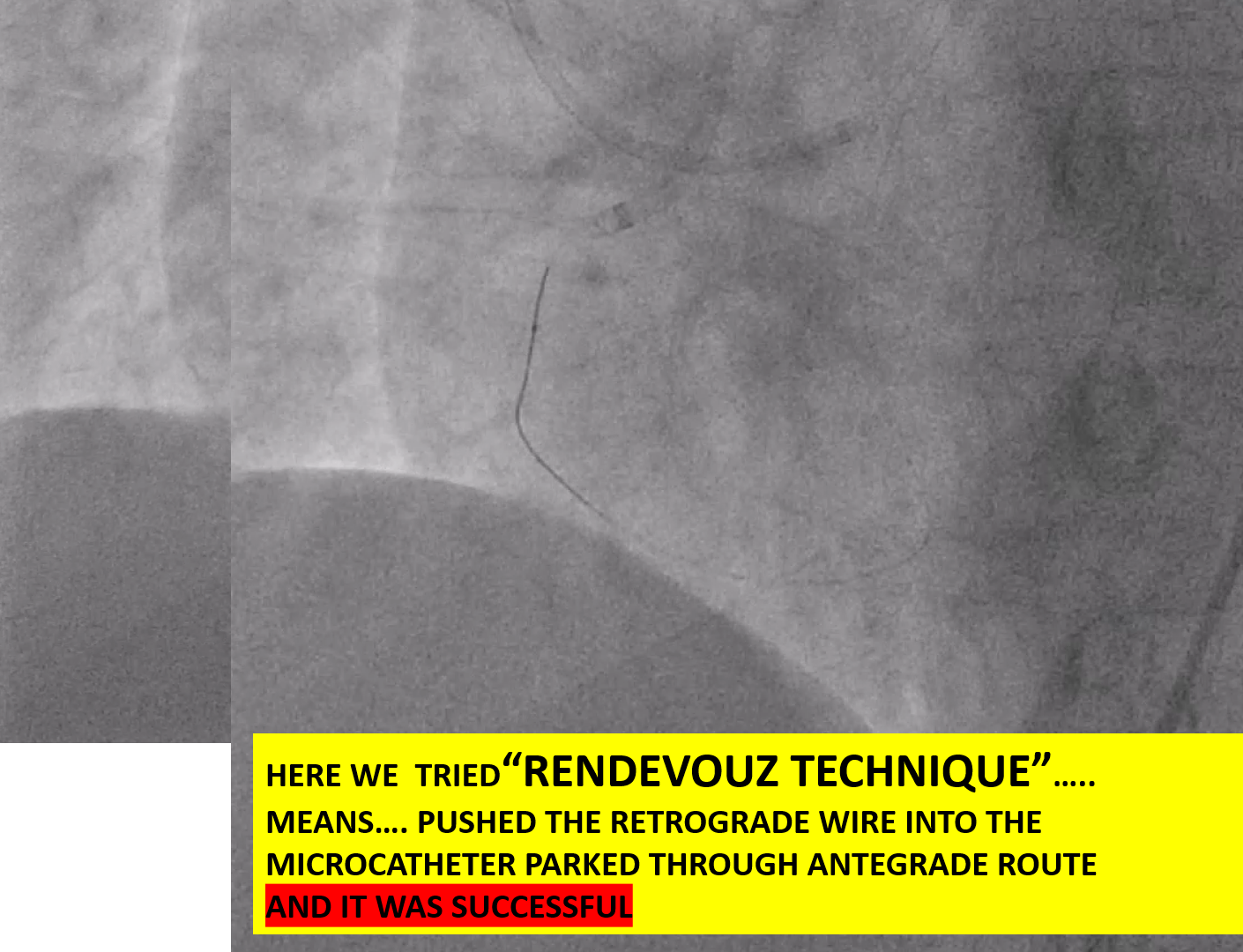
PTCA with Retrograde Rendezvous for Chronic Total Occlusion (CTO)An individual with a stubborn Chronic Total Occlusion (CTO) in the RCA (Right Coronary Artery) initially underwent a failed antegrade percutaneous transluminal coronary angioplasty (PTCA). Despite multiple wire attempts (e.g., CROSSIT 200, PILOT 150), the procedure was aborted due to a spiral dissection.A month later, a second attempt was made using a more advanced approach. The steps were as follows:Retrograde Access: The interventional team chose a retrograde approach, navigating a wire and microcatheter through collateral vessels to reach the RCA distal to the blockage.Antegrade Access: Simultaneously, an antegrade wire was advanced from the proximal end of the RCA to the blockage site.Rendezvous: The retrograde and antegrade wires were "kissed" at the site of the CTO. This crucial step, known as the rendezvous technique, allowed the antegrade wire to be precisely guided.Final Crossing: The antegrade wire was then advanced through the antegrade microcatheter, alongside the retrograde wire, finally penetrating the true lumen distal to the CTO.Revascularisation: Once the path was clear, the retrograde wire was removed. The RCA was then successfully revascularized with balloon dilations and the deployment of two stents.


Case Summary
RETROGRADE WITH GRADE 1 OR 2 COLLATERALLS IS CHALLENGINGWhen a microcatheter can not cross RETROGRADELY INTO THE RECIPIENT VESSEL, THERE IS DIFFICULTY TO CROSS the CTO SEGMENTHYBRID APPROACH AND TECHNIQUES LIKE RENDEVOUZ ARE VERY EFFECTIVE