CASE20250708_001
Alloy Jaket Calcium Tunnel: Calcified Lesion With Nearly No Expansion Stent
By Yu-Cheng Kao
Presenter
Yu-Cheng Kao
Authors
Yu-Cheng Kao1
Affiliation
Cheng Hsin General Hospital, Taiwan1
View Study Report
CASE20250708_001
Complex PCI - Calcified Lesion
Alloy Jaket Calcium Tunnel: Calcified Lesion With Nearly No Expansion Stent
Yu-Cheng Kao1
Cheng Hsin General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
This is a 70 years old female with Hypertension, Diabetes Mellitus, Dyslipidemia, and 3-vessel-disease post LAD and LCX stenting at a local hospital.She got angina deterioration in recent 3 months and received coronary angiography in the local facility. After that, the patient was refered to our center for balloon un-dilatable Severe In-Stent Restenosis.

Relevant Test Results Prior to Catheterization
The patient's echocardiography showed the LVEF 68% with apical anteroseptal hypokinesia.
 Echo submmit.pptx
Echo submmit.pptx
Relevant Catheterization Findings
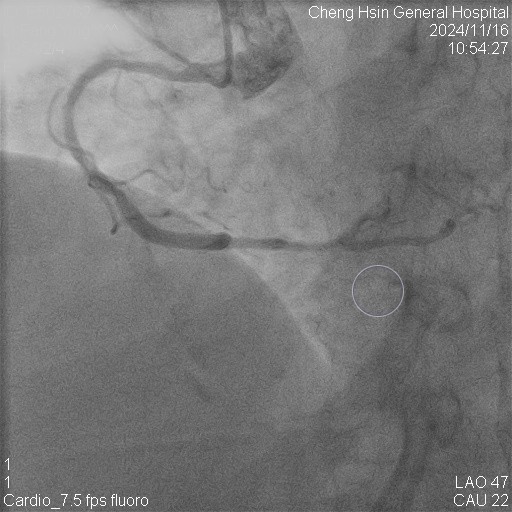
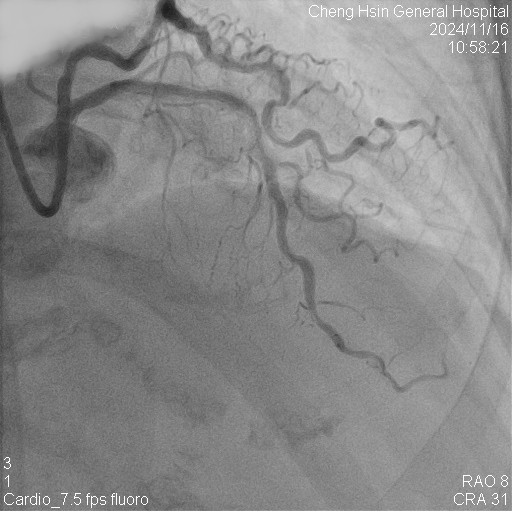
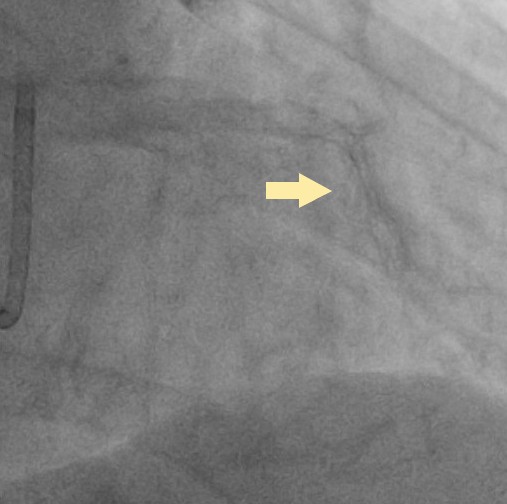
The RCA was calcified but no significantly severe stenosis.The LCX was calcified with mild stenotic lesion and a patent old stent.The LAD was severely calcified with an under-expanded old stent at middle to distal part. The lesion was also severely stenotic. The proximal to middle LAD had moderately stenotic lesion with calcification also.
Interventional Management
Procedural Step
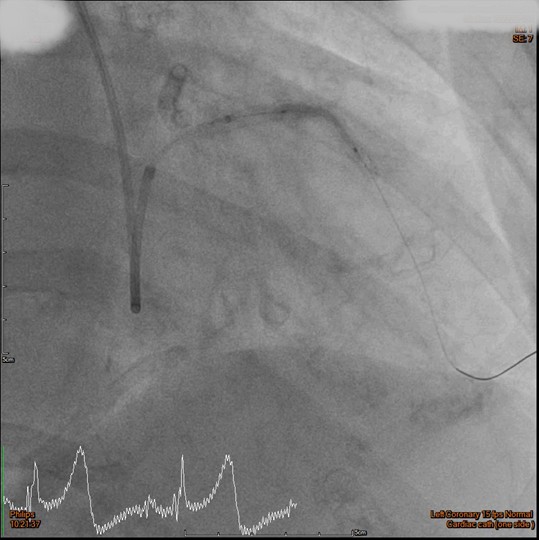
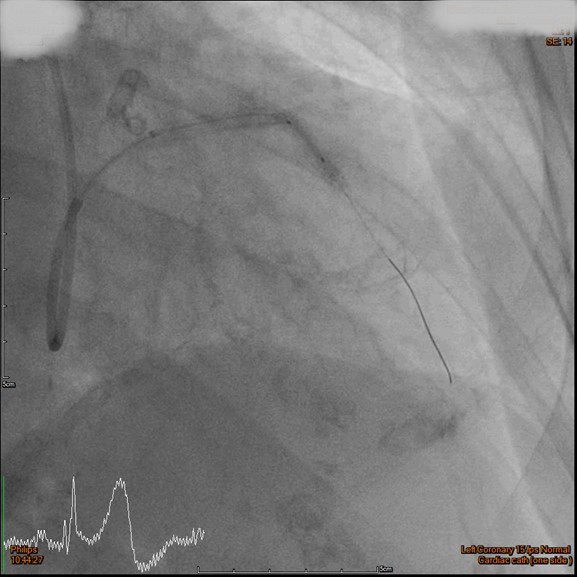
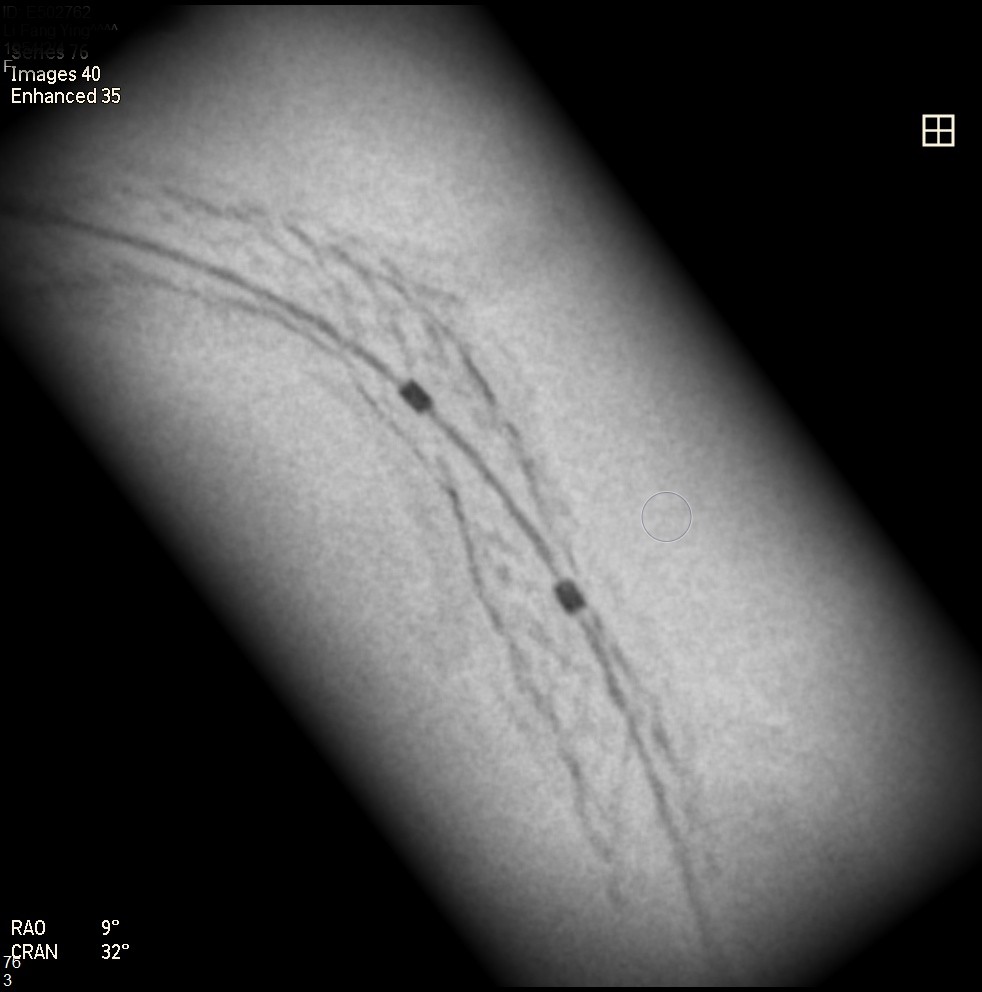
Initially, we tried to insert IVUS catheter but unable to cross the lesion. We tried a NC balloon but unable to cross it also.Hence, we used rotational atherectomy with 1.5mm burr. However, the burr was unable to cross lesion even in high speed and entrapped in the stent.We removed the burr in guide extension catheter then the NC balloon could cross the lesion. The IVUS cather could also cross it with guide extension catheter support. The stent was almost not expanded. We tried NC balloon high pressure dilation but balloon slippage and burst. The lesion was still un-dilatable. We insert cutting balloon which avoided slippage but remained burst. We escalated the burr size to 1.75mm. The larger burr was not stucked but still unable to cross lesion. Besides, the larger burr causing slow blood flow. After adenosine injection, the patient's blood flow recovered. We reduced the burred size to 1.25mm which cross the lesion once but entrapped while doing polishment. After burr retrieval, we used NC balloon high pressure dilation. The balloon bursted but the lesion remained un-dilatable.Finally, the lithotrypsy balloon could cross the lesion and eliminate 80 pulses. The lesion was expanded much well. The IVUS showed the old stent was expanded and calcium was cracked. We deployed a new stent for old one destruction and proximal dissection. The final IVUS image showed epansion and apposition were accpetable.

Case Summary
The best way to deal with such kind of lesion is prevention. To use intravascular image guidance is very important in complex PCI. Do not insert stent if insufficient lesion preparation. Uncrossable, thick calcium and nodules, limit the efficacy of lithotripsy balloon and often causing IVL balloon rupture. Before inserting the lithotripsy balloon, we might need rotational atherectomy to modified the lesion or the road to the lesion. Larger burr size makes slow flow while smaller one let you stuck in such kind of stent jacket calcium tunnel.The Rotatripsy had demonstrated effectiveness and safety in addressing severe calcified coronary artery disease.