CASE20250724_002
Standing at the Crossroad: A Challenging Case With Stumpless Left Anterior Descending Artery Bifurcation Chronic Total Occlusion
By Hsiao-Tse Tu
Presenter
Hsiao-Tse Tu
Authors
Hsiao-Tse Tu1
Affiliation
Taichung Veterans General Hospital, Taiwan1
View Study Report
CASE20250724_002
Complex PCI - CTO
Standing at the Crossroad: A Challenging Case With Stumpless Left Anterior Descending Artery Bifurcation Chronic Total Occlusion
Hsiao-Tse Tu1
Taichung Veterans General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
The patient was a 83-year-old male with past medical history of ischemic stroke and vascular cognitive impairment, who had no habit of cigarette smoking. He ever experienced STEMI and received primary PCI for RCA in 2025/06. LAD-os stumpless CTO was also found at that time. One month later, the patient was admitted once again for staged PCI for LAD.
 003110218I_003.AVI
003110218I_003.AVI
003110218I_010.AVI
003110218I_021.AVI
Relevant Test Results Prior to Catheterization
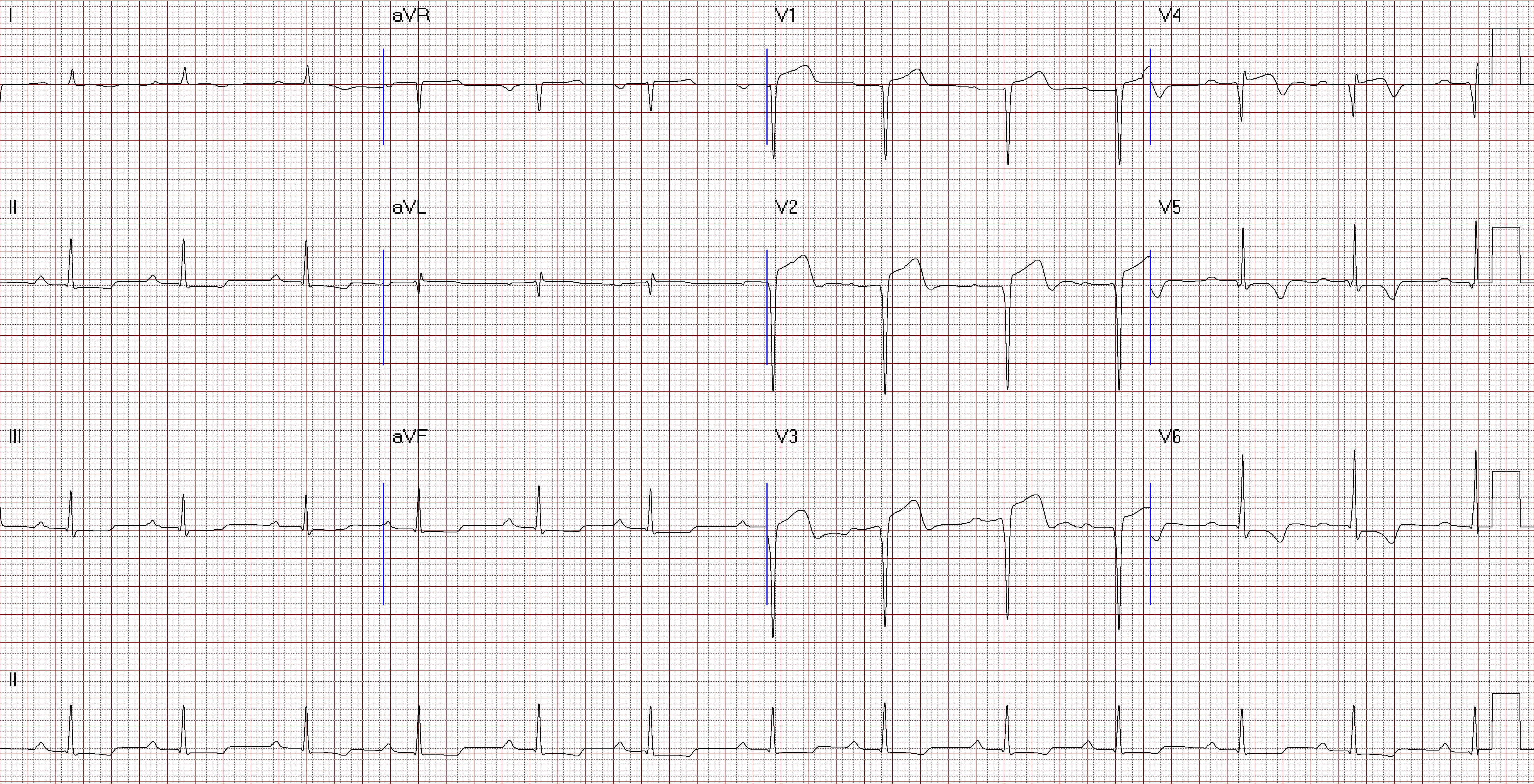
Lab data showed fair renal function and mild anemia. Chest X ray found no cardiomegaly or pulmonary congestion. ECG showed persistent ST elevation over anterior leads. Echocardiogram disclosed general LV hypokinesia with reduced LVEF about 30% and LV aneurysm formation.

I2-26_19.avi
Relevant Catheterization Findings
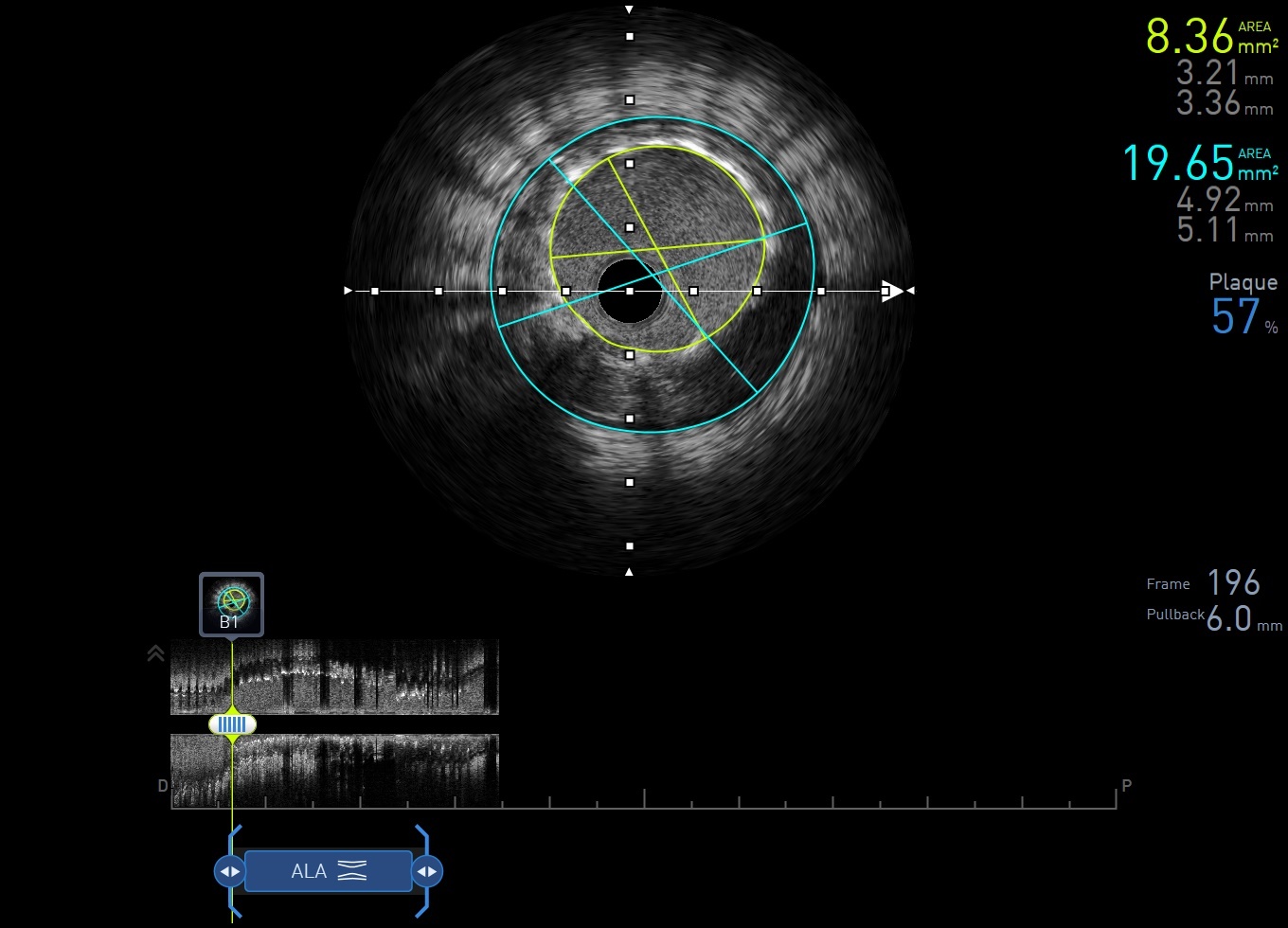
Catheterization found LAD-os CTO with collateral circulation from LCA and RCA. The largest collateral artery was originated from PL branch. Previous stent over RCA-m was found underexpanded with IVUS. Before proceeding to LAD CTO, we fixed underexpanded stent first with 4.0 x 12mm NC BC.
003110218I_007.AVI
003110218I_008.AVI
Interventional Management
Procedural Step
We did retrograde approach for LAD-os CTO. With Finecross microcatheter support, Sion Black was advanced to diagonal branch through PL branch. Then we engaged LCA with EBU 3.5 x 6 Fr GC and changed Sion Black to Fielder XTA. With Finecross support, Fielder XTA passed through LAD-os to diagonal CTO lesion and was advanced into LM, and it was confirmed by IVUS. Retrograde system was converted to antegrade with Tip-in technique, and antegrade microcatheter was advanced to diagonal branch. We then used IVUS to confirm the stump position of LAD-PMJ CTO. We once tried to use Crusade double lumen catheter and IVUS for stump wiring but 6 Fr GC was not large enough for using both devices simultaneously. We then marked the location of stump on angiogram, and tried to wire with Fielder XTA. Finally, Fielder XTA passed CTO stump with Finecross support, then we changed Fielder XTA to Gaia 1 and it was advanced to distal LAD. LAD CTO lesion was dilated with 1.0 and 2.0mm BC. IVUS showed that we were all the way in true lumen except a very short part in LAD-d. LAD-os to LAD-m lesion was scaffolded with 2.5 x 48mm DES and it was dilated with 3.0 x 12mm NC BC. For angiogram showed distal stent edge dissection and contrast leakage from second diagonal branch, we checked echocardiogram but found no pericardial effusion and vital signs were stable. Distal stent edge dissection was scaffolded with 2.5 x 12mm DES and LAD-d small vessel was dilated with 1.5mm BC. Final angiogram showed good result.
003110218I_084.AVI
003110218I_003.AVI
003110218I_259.AVI
Case Summary
1. Combining good antegrade and retrograde techniques is extremely important for complicated CTO PCI.2. Tip-in technique helps to convert the system from retrograde to antegrade when externalization is unfeasible or undesirable. 3. It takes at least 7 french guiding catheter for using microcatheter and intravascular image simultaneously for real-time intravascular ultrasound-guided wiring.