CASE20250728_001
An Interesting Case Report: Coronary Embolism From Aortomitral Intervalvular Fibrosa Pseudoaneurysm in a Patient Following Aortic Valve Replacement and Mitral Valve Repair for Infective Endocarditis
By Lalitwadee Kingmaiklang, Kittichok Jonggonsuwan, Wittawat Wattanasiriporn
Presenter
Lalitwadee Kingmaiklang
Authors
Lalitwadee Kingmaiklang1, Kittichok Jonggonsuwan1, Wittawat Wattanasiriporn1
Affiliation
Rajavithi Hospital, Thailand1
View Study Report
CASE20250728_001
ACS/AMI - ACS/AMI
An Interesting Case Report: Coronary Embolism From Aortomitral Intervalvular Fibrosa Pseudoaneurysm in a Patient Following Aortic Valve Replacement and Mitral Valve Repair for Infective Endocarditis
Lalitwadee Kingmaiklang1, Kittichok Jonggonsuwan1, Wittawat Wattanasiriporn1
Rajavithi Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
A Thai 29-year-old man with history of Severe AR and severe MR due to Infective endocarditis S/P Bileaflet Aortic valve replacement with Mitral valve repair in 2022 presented to emergency department with acute chest pain 4 hour. He had history of discontinuation of warfarin 3 months prior to presentation.
V/S: T 36.2 C, BP 120/66 mmHg, PR 85 bpm, RR 17 /min. Heart : Seen surgical scar at midchest, no murmur, valve’s click heard at aortic area, Lung: clear both lungs.
V/S: T 36.2 C, BP 120/66 mmHg, PR 85 bpm, RR 17 /min. Heart : Seen surgical scar at midchest, no murmur, valve’s click heard at aortic area, Lung: clear both lungs.
Relevant Test Results Prior to Catheterization
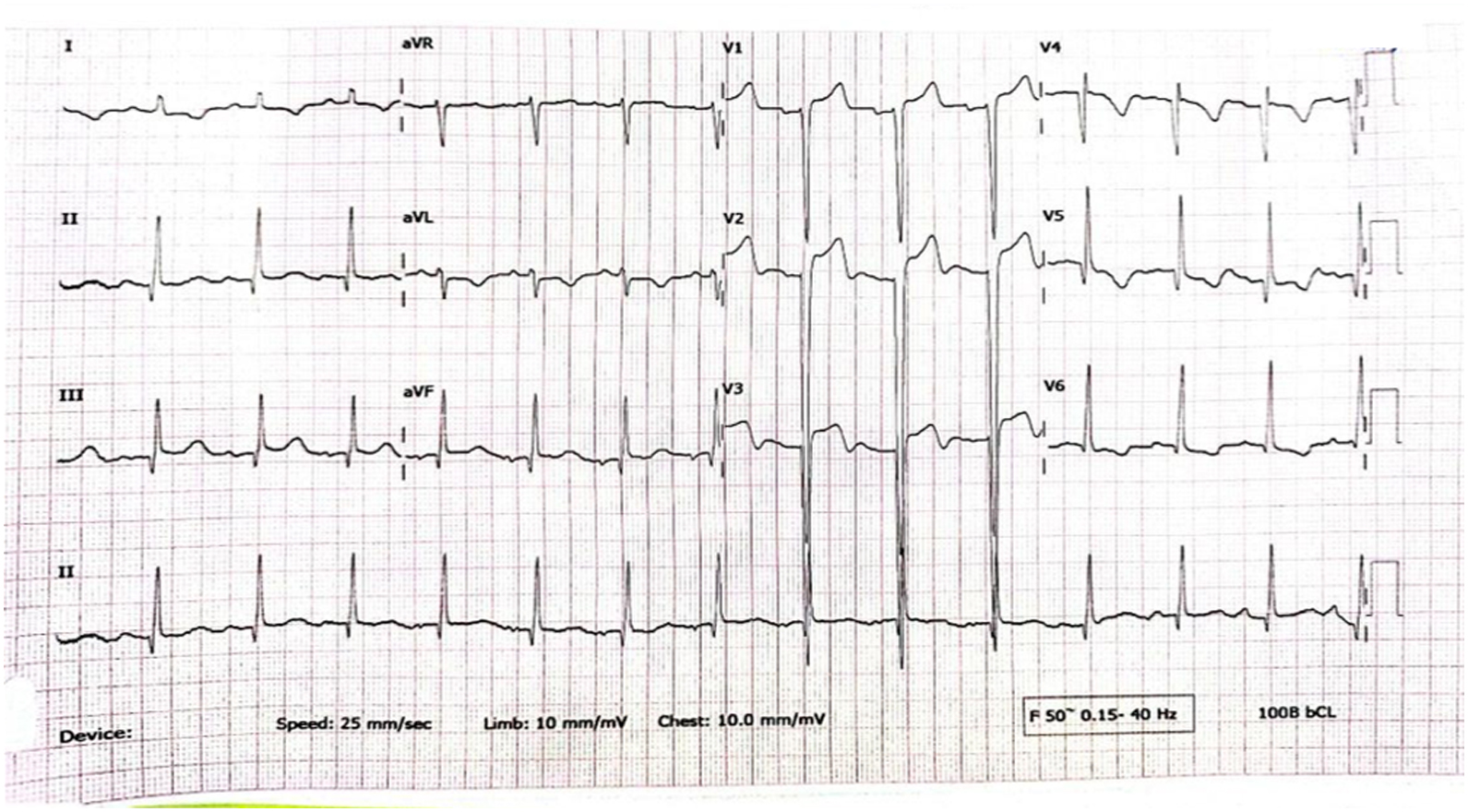
EKG showed normal sinus rhythm with ST segment elevation at V1-3, inverted T wave at V4-6, I,aVL.
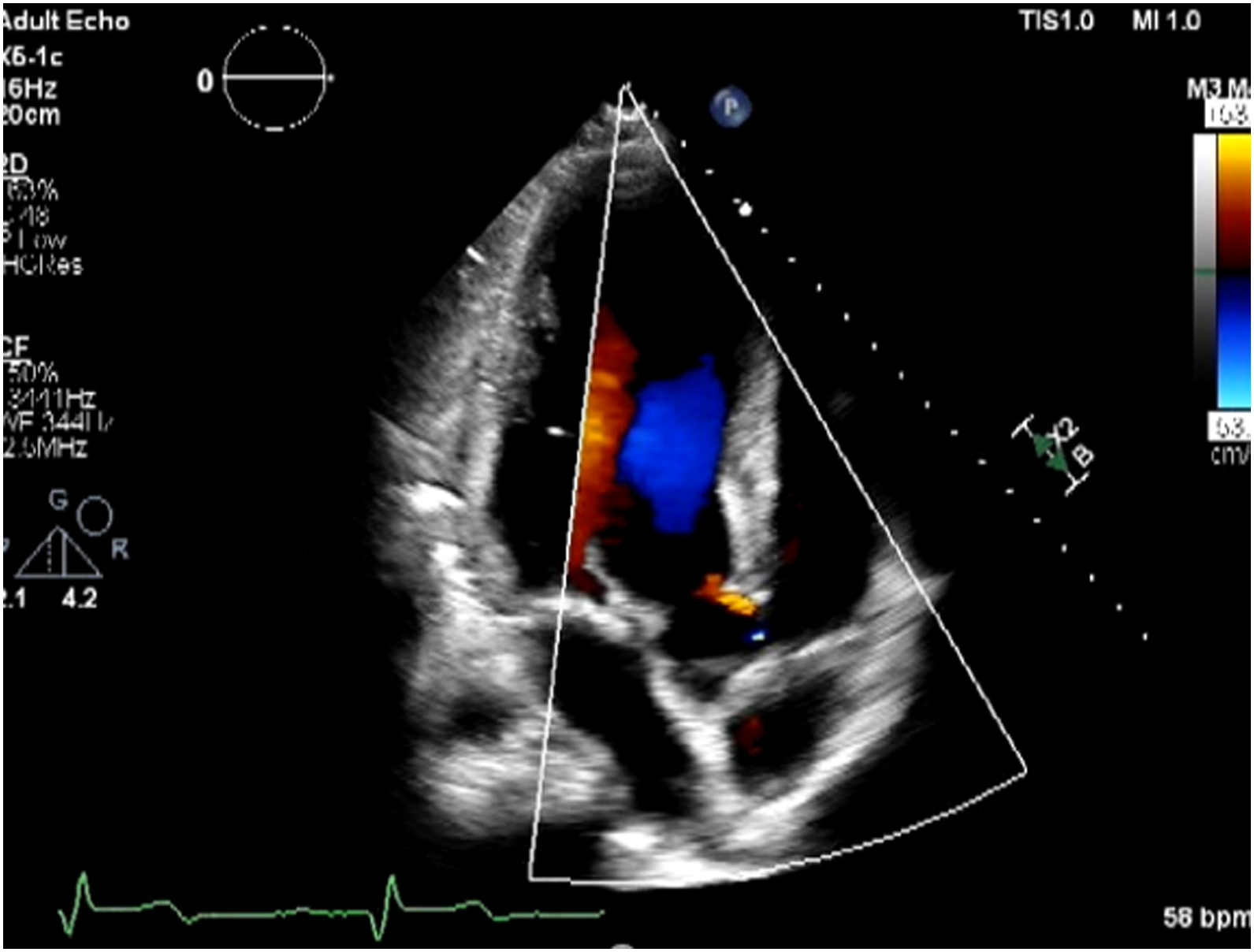
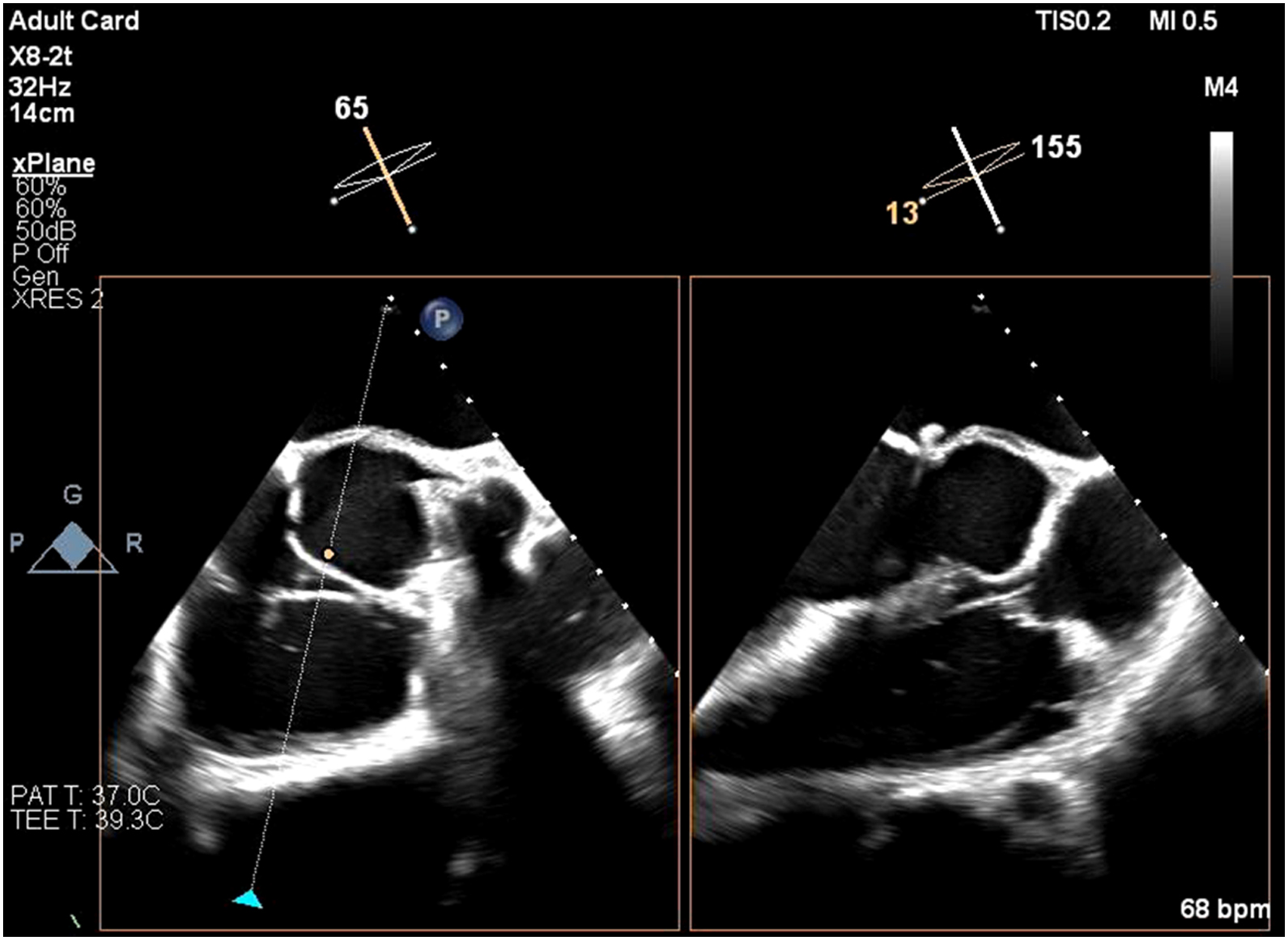
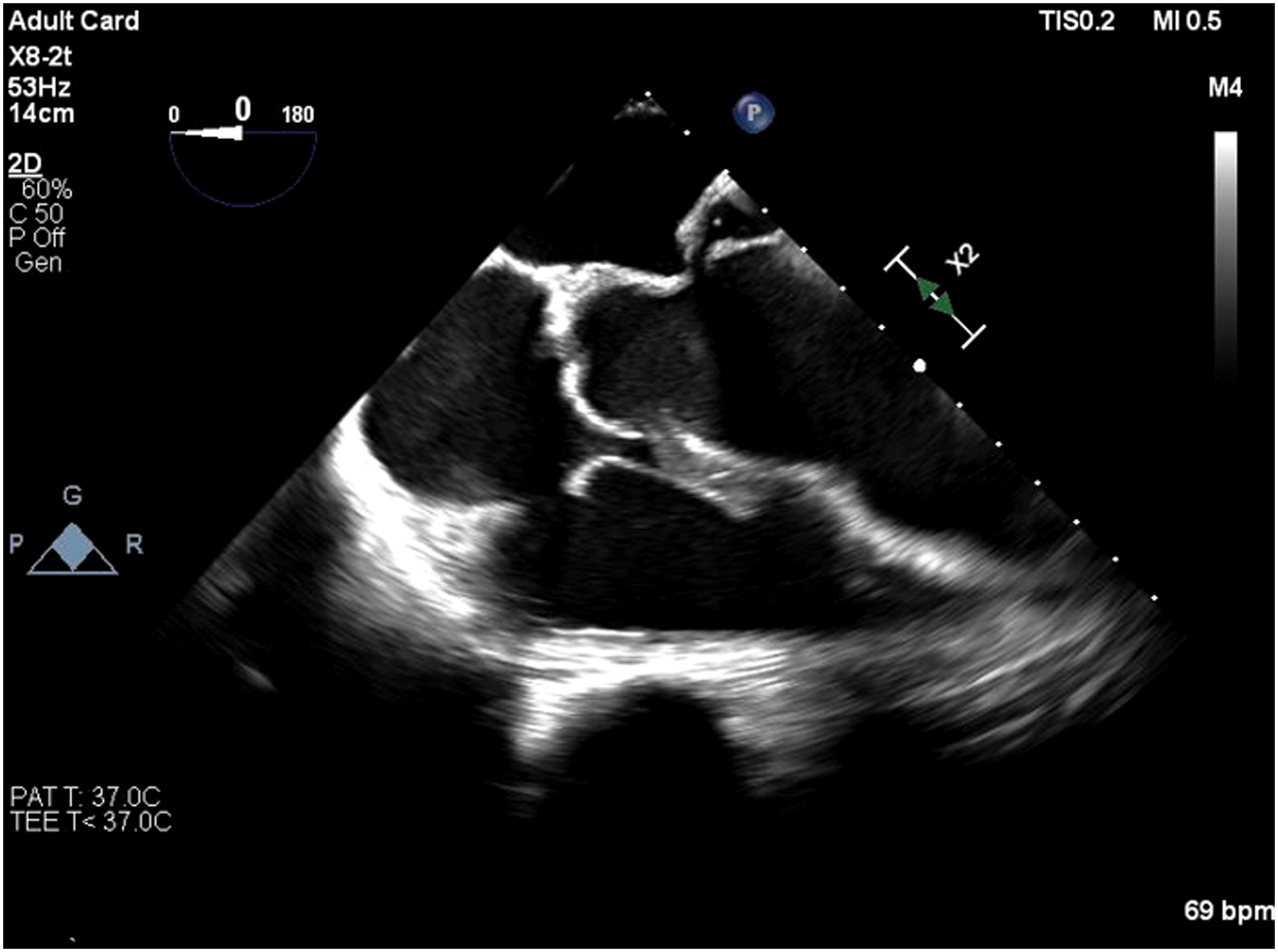
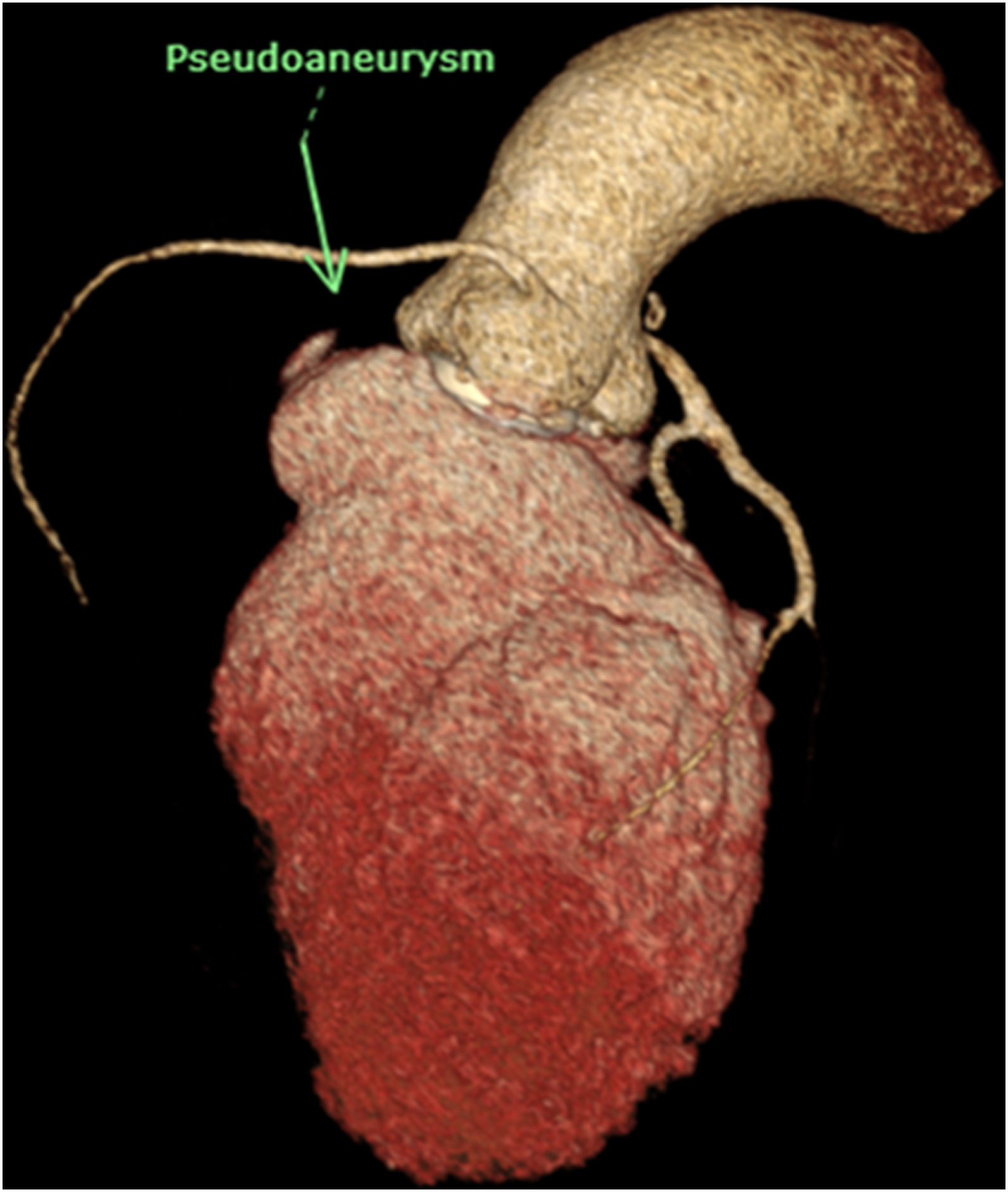
Echocardiogram showed impaired LV systolic function, global wall hypokinesia, normal prosthetic aortic valve function with mild paravalvular leakage and bulging of aortomitral intervalvular fibrosa, suspected
Aortomitral intervalvular fibrosa aneurysm.
CT cardiac revealed pseudoaneurysm of the aortomitral intervalvular fibrosa with laminated thrombus with no LAA thrombus visualized.

Relevant Catheterization Findings
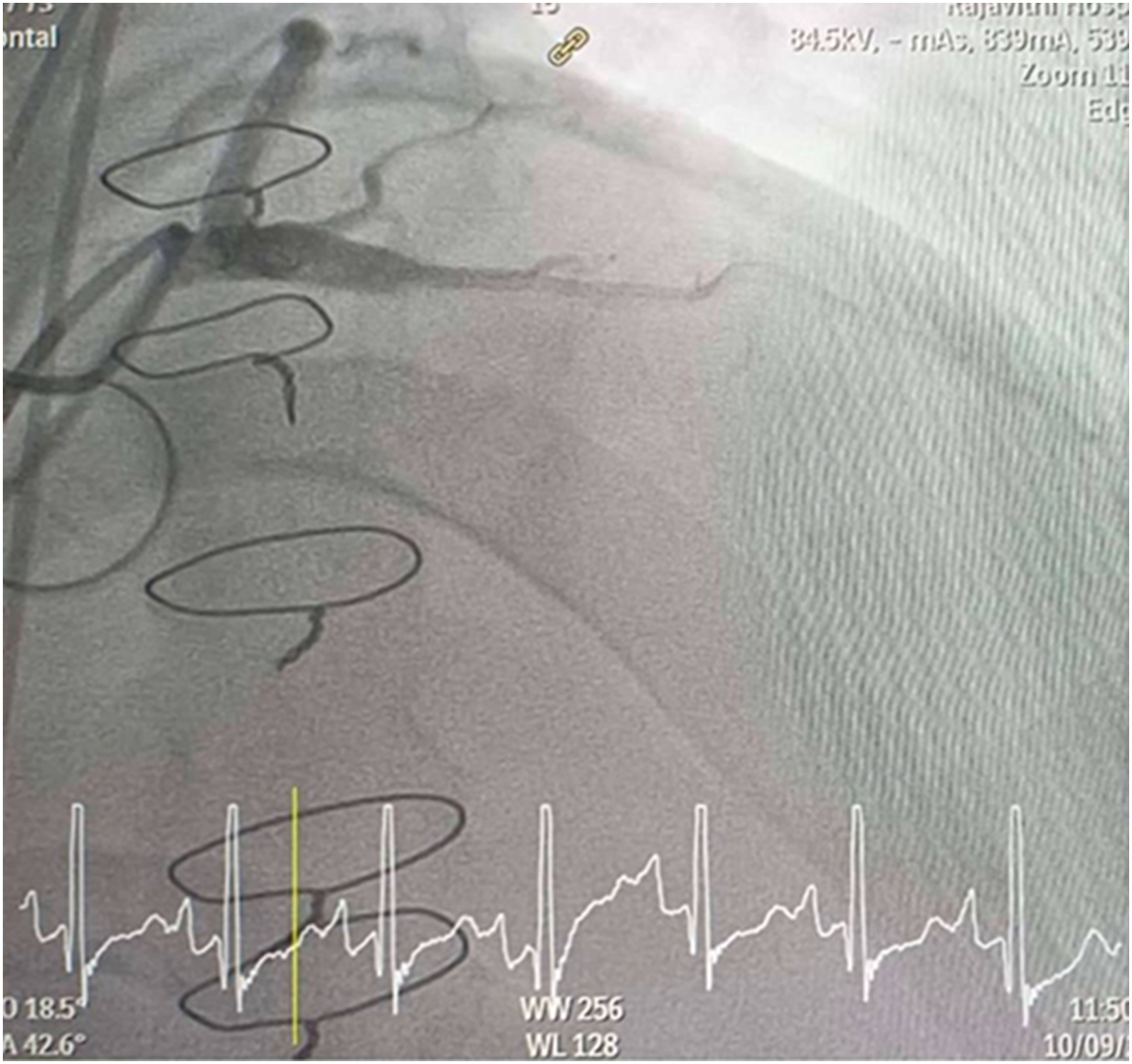
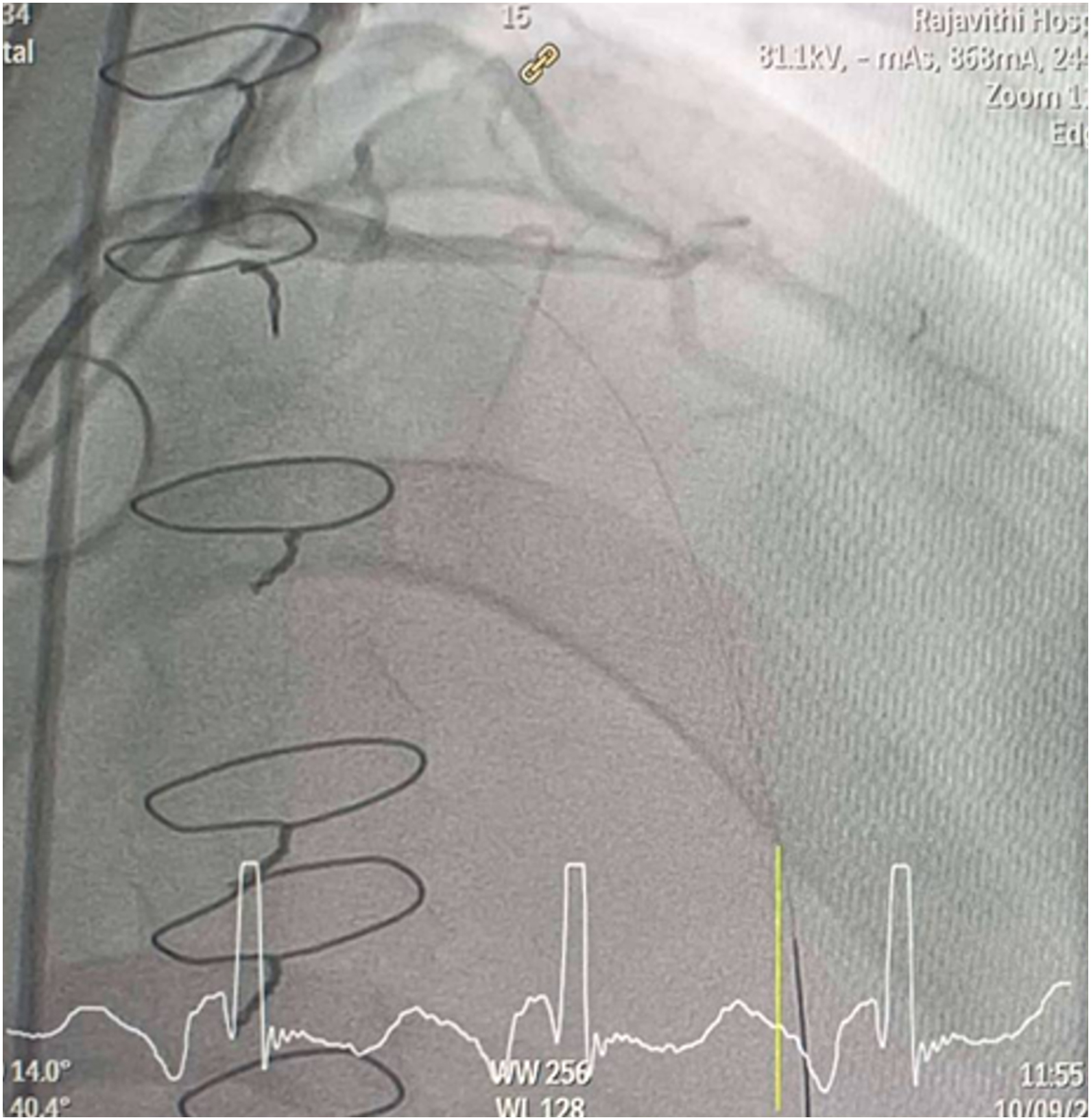
CAG was performed with right femoral approach with JL 4.0/7 Fr, JR 4.0/6 Fr diagnostic catheter showed
Right dominant
LM : mild irregular, non significant stenosis.
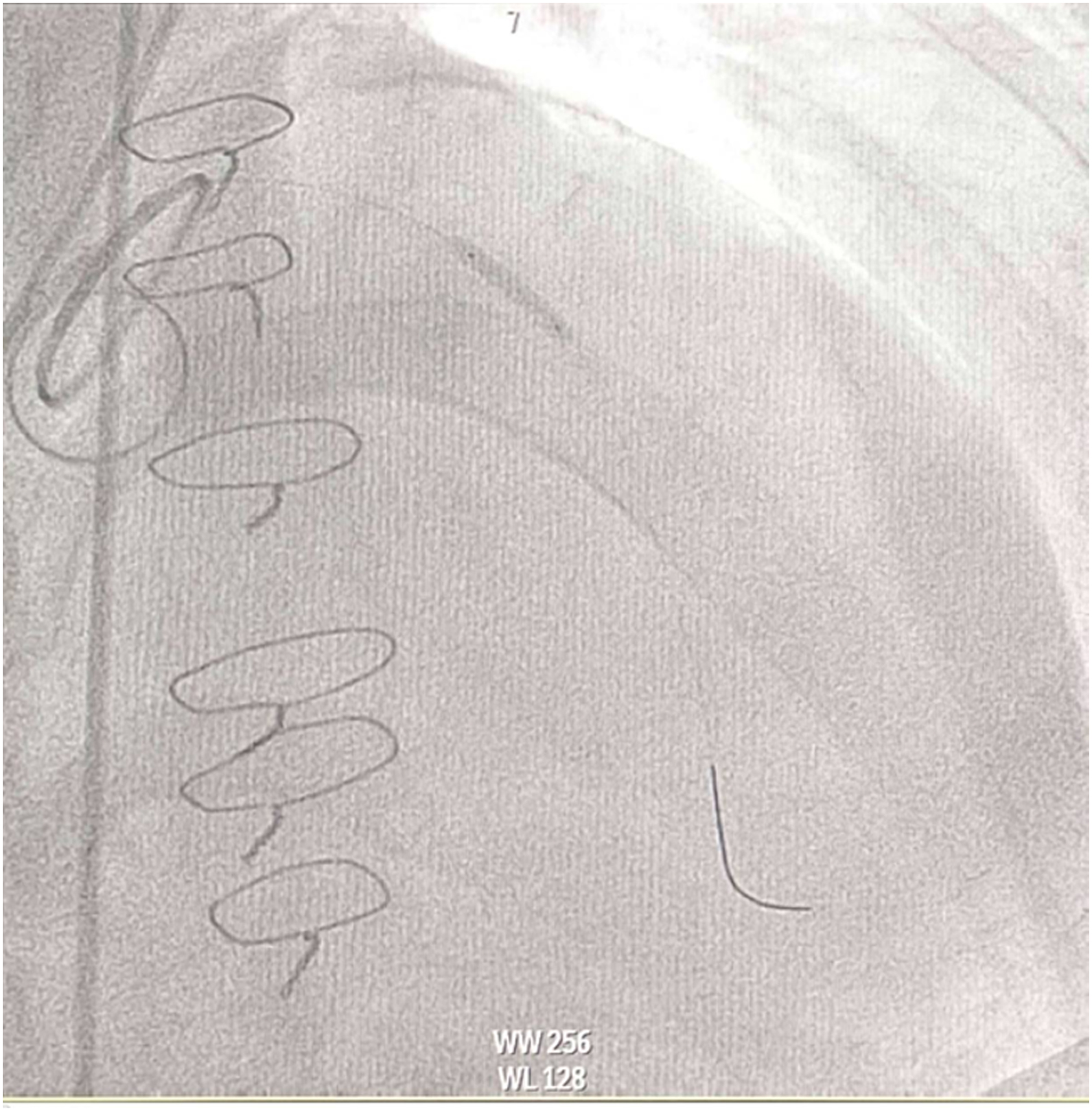
LAD : total occlusion mLAD.
LCx : mild irregular, non significant stenosis.
RCA : non significant stenosis.
Interventional Management
Procedural Step
Procedural Step
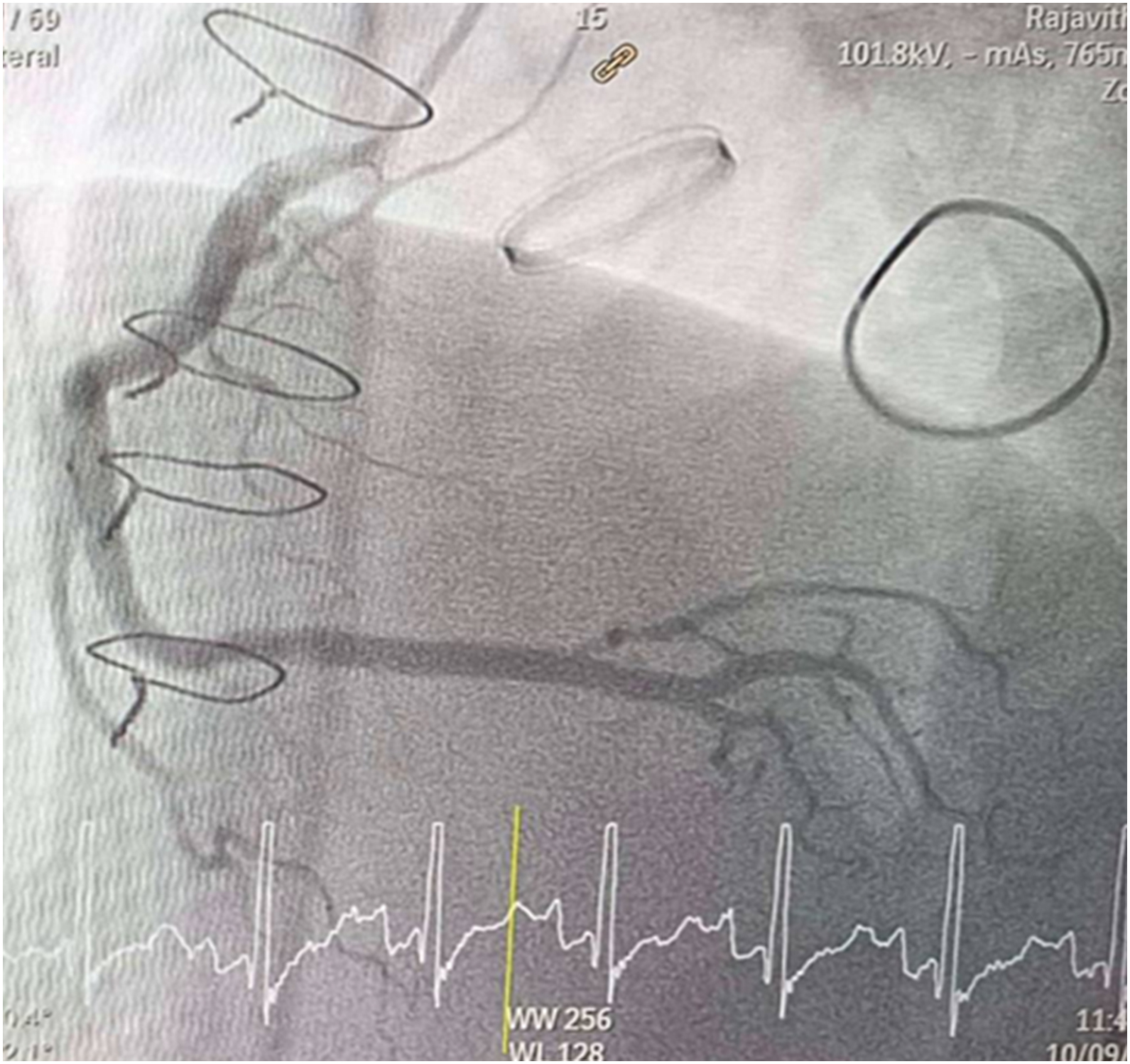
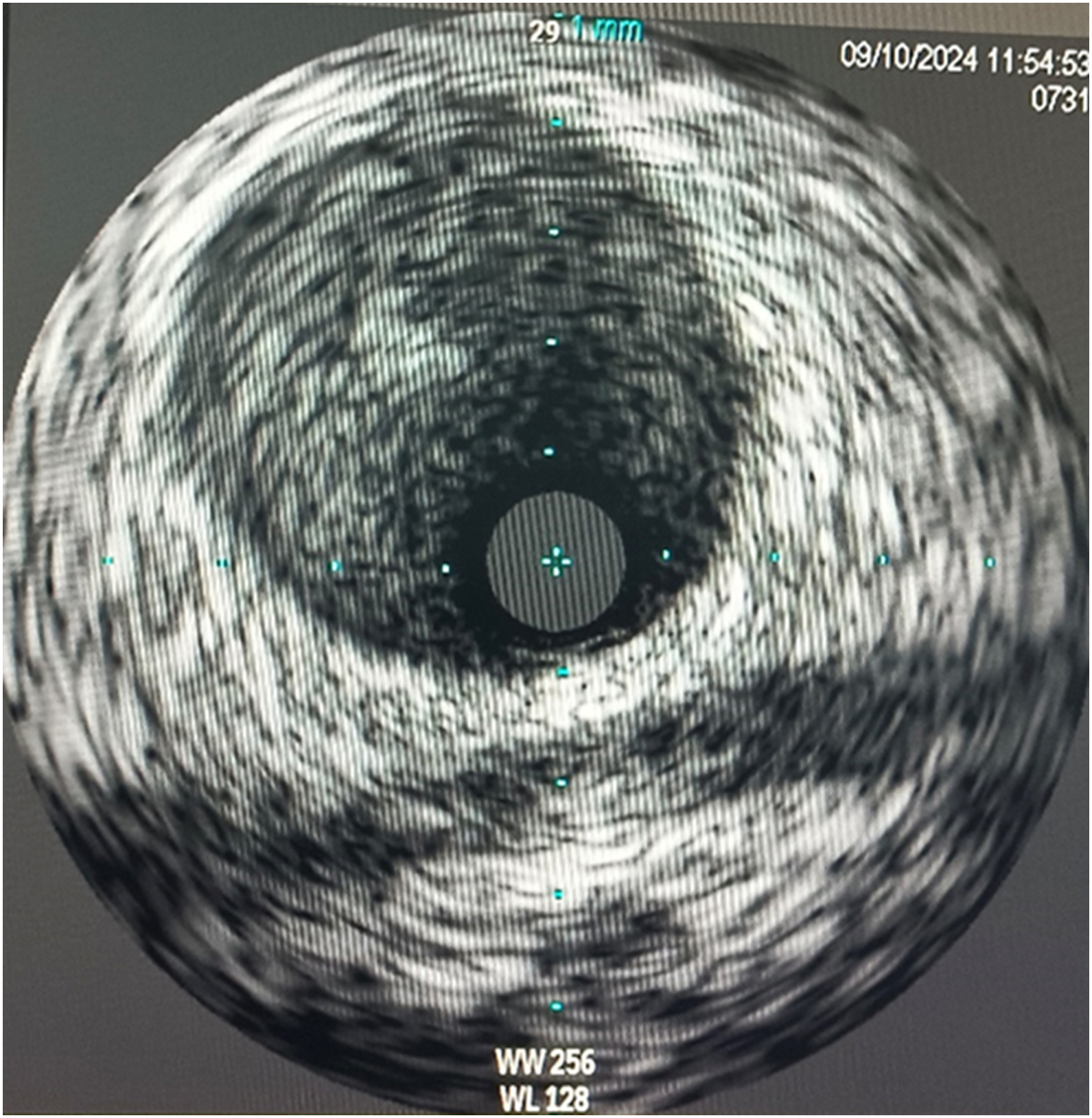
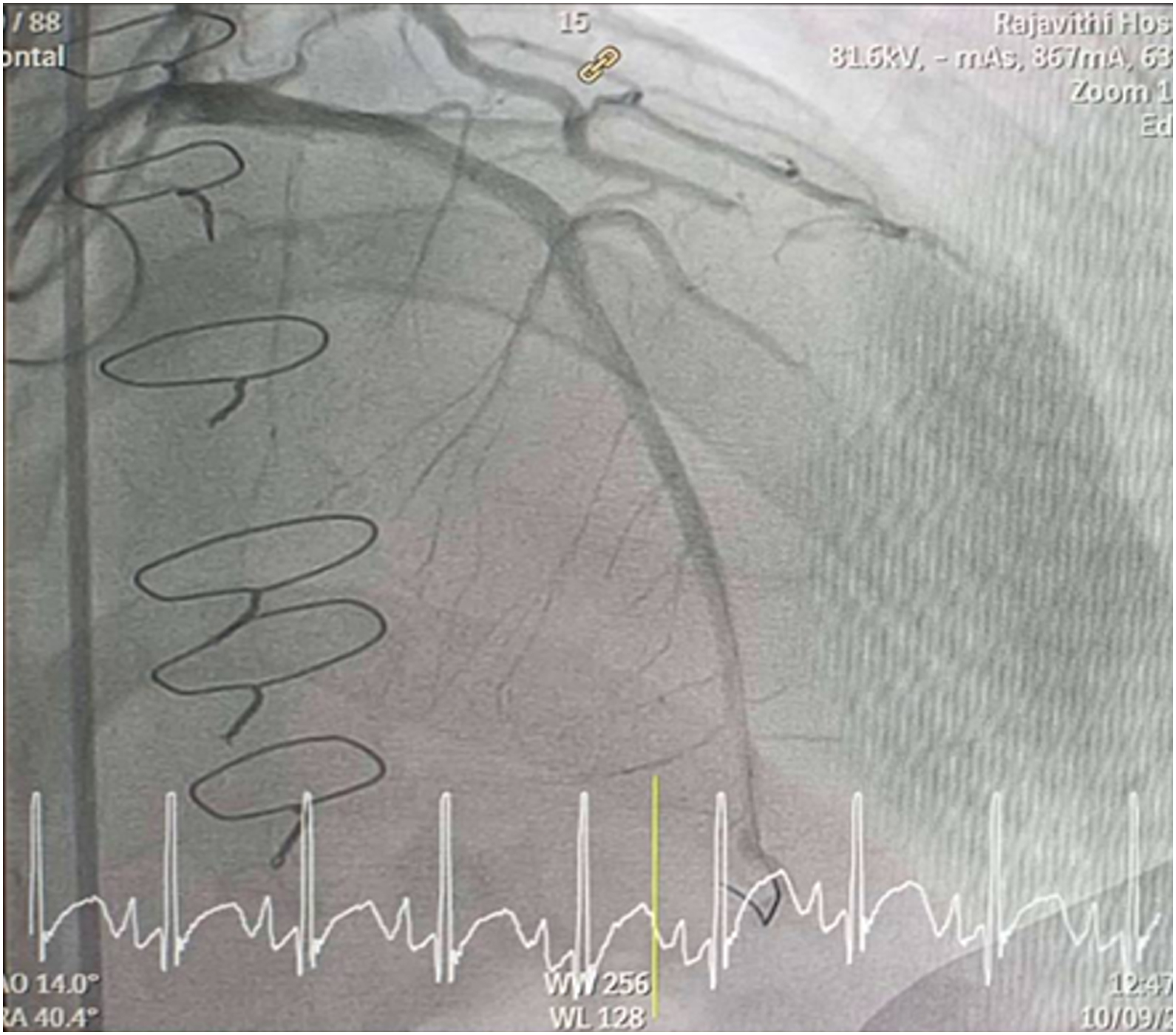
Inserted Sion wire and thrombuster to LAD revealed multiple red clots.SC balloon 2.0 x 15 mm, then 2.5 x 15 mm, was inflated at mLAD up to 12 atm. IVUS insertion to LAD revealed vessels’ size LM 5-5.5 mm, pLAD 4-4.5 mm, mLAD 3-3.5 mm with intraluminal thrombus, dLAD 2.75-3 mm. Multiple inflations were done at mLAD with SC balloon 2.5 x 15 mm. After multiple SC balloon inflations, the CAG revealed slow flow phenomenon. Then, the operator performed thrombus aspiration, multiple SC balloon 2.0 x 15 mm inflation and gave IC integrillin 3.4 ml. The final angiogram was acceptable result. The anticoagulant was given after CAG. Chest pain was subsided and hemodynamic parameters remained stable. EKG recorded after angiography showed resolution of ST elevation at V1-3. Later, the patient was discharged with warfarin. The Aortomitral intervalvular fibrosa repair surgery was planned due to embolic complication.
Case Summary
1. Coronary embolism can be considered as a rare cause of STEMI.
2. Diagnosis of coronary embolism remains challenging, requires a high level of suspicion, comprehensive angiographic evaluation and other imaging modalities.
3. Anticoagulant after prosthetic valve implantation should be continue lifelong to prevent further thromboembolic events.
4. We report an extremely rare case of Aortomitral intervalvular fibrosa pseudoaneurysm with coronary embolism. Due to its very low incidence, it presents both a diagnostic and therapeutic challenge.
5. Intravascular imaging is beneficial in determinating the mechanism of CAD, informing therapeutic strategy and confirming effective treatment of PCI.