CASE20250728_002
Hydrodynamic Recanalization with Intraplaque Contrast Injection Facilitating True Lumen Crossing in a Severely Calcified Left Anterior Descending Chronic Total Occlusion
By Alvaro Contreras, Jose Pablo Sonqui, Joel EStrada
Presenter
Alvaro Contreras
Authors
Alvaro Contreras1, Jose Pablo Sonqui1, Joel EStrada 1
Affiliation
National Medical Center XXI Century, Mexico1
View Study Report
CASE20250728_002
Complex PCI - CTO
Hydrodynamic Recanalization with Intraplaque Contrast Injection Facilitating True Lumen Crossing in a Severely Calcified Left Anterior Descending Chronic Total Occlusion
Alvaro Contreras1, Jose Pablo Sonqui1, Joel EStrada 1
National Medical Center XXI Century, Mexico1
Clinical Information
Relevant Clinical History and Physical Exam
A 66-year-old man with a history of hypertension and type 2 diabetes mellitus diagnosed 10 years ago, and a past history of tobacco use (currently discontinued), with no prior cardiovascular history, was evaluated for a 4-month history of typical angina refractory to medical therapy. Physical examination revealed no pathological cardiovascular findings.
Relevant Test Results Prior to Catheterization
Functional ischemic stratification with SPECT, which demonstrated moderate inferior ischemia and severe anteroseptal ischemia. Baseline transthoracic echocardiography revealed a left ventricular ejection fraction (LVEF) of 40%, without evidence of significant valvular disease.

Relevant Catheterization Findings
Coronary angiography showed multivessel coronary artery disease, including a severe, long stenosis in a large posterolateral branch of the right coronary artery (RCA), diffuse severe disease in the left circumflex artery (LCX), and a severely calcified chronic total occlusion (CTO) of the mid left anterior descending artery (LAD).
 Angio CTO.mov
Angio CTO.mov
Angio CTO 2.mov
Angio CTO CC.mov
Interventional Management
Procedural Step
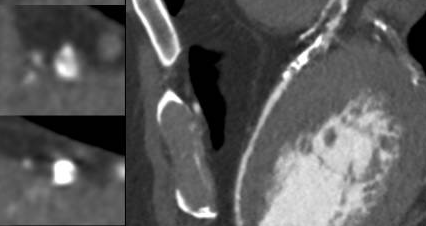
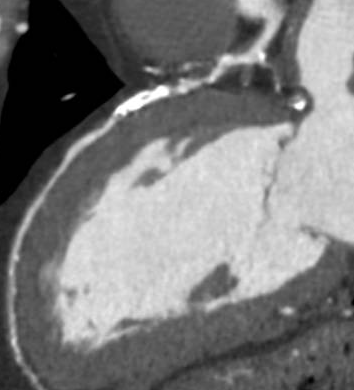
Antegrade wire escalation was attempted using a Corsair ProXS 135 cm (Asahi Intecc) and multiple guidewires, including the Fielder XT, Gaia Next 2, and Gaia Next 3 (Asahi Intecc). However, none of the guidewires were able to successfully cross the occlusion. Hydrodynamic recanalization (HDR) was then attempted. Followig a 0.5 cc tip injection of contrast no progress was achieved. A second HDR injection was performed, after which a Gaia Next 2 guidewire successfully crossed the CTO to the distal LAD. However, the Corsair Pro XS microcatheter failed to cross the distal cap and became fatigued during manipulation. An anchoring technique with a 1.5 × 15 mm SC balloon in the septal branch was performed in an attempt to support crossing of the Caravel microcatheter (Asahi Intecc), but the distal cap remained uncrossoable. Caravel microcatheter was left within the CTO body, and a floppy Rotawire Drive guidewire (Boston Scientific) was advanced to the distal LAD. Rotational atherectomy was then carried out with a 1.5 mm burr using the Rotapro system (Boston Scientific) at 180,000–200,000 rpm for a total of 8 minutes. IVUS imaging using Opticross (Boston) confirmed true lumen crossing, presence of circumferential calcification, reverberation as well as superficial plaque fractures. Sequential predilatation with a Wolverine cutting ballon was performed and then definite stenting was accomplished with a 3.5x48 mm and 4.0x38 mm Synergy XD extending from mid LAD into left main
COMPLEX PCI CASE ALVARO CONTRERAS.mp4
Case Summary
This case highlights the value of hydrodynamic recanalization using intraplaque contrast injection as a tool to facilitate true lumen crossing in complex, calcified chronic total occlusions when standard techniques fail. It may serve as a strategic bridge to successful atherectomy and stenting in challenging anatomy.