CASE20250730_001
Coronary [D]emon Hunter
By Sze Wah Lai
Presenter
Sze Wah Lai
Authors
Sze Wah Lai 1
Affiliation
CMC, Hong Kong, China1
View Study Report
CASE20250730_001
ACS/AMI - ACS/AMI
Coronary [D]emon Hunter
Sze Wah Lai 1
CMC, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
55 years old lady with history of multinodular goiter.
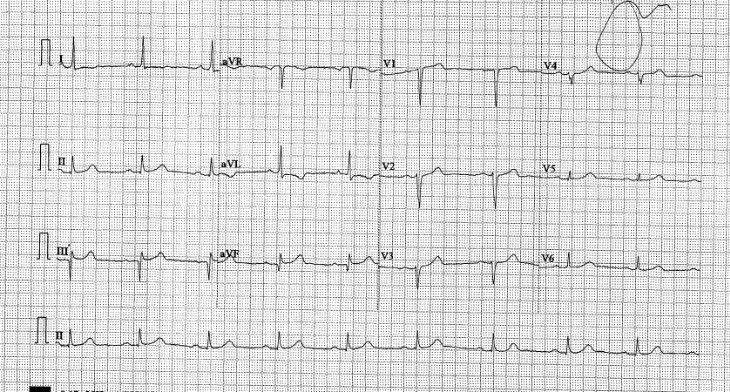
Complained of sudden onset chest discomfort since 8:00 in the morning. no back radiation, pain persistentECG in A&E Department showed 1mm ST elevation over II, III, AVF, with reciprocal depression over AVLEchocardiogram showed mid to apical anteroseptal marked hypokinesia, no aortic flap or aortic regurgitation Haemodynamic was stable and on high side Patient was brought to Cath lab for primary PCI
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
coro showed normal RCA, LCx. but LAD noted to have Spontaneously dissection flap along the LAD from proximal to distal LAD with TIMI 1 flow.
 CTL CORO1.mov
CTL CORO1.mov
CTL Coro2.mov
Interventional Management
Procedural Step
Right radial approach for angiogram which showed long LAD spontaneous coronary dissection We decided to switch to Right femoral approach with 7F shealth and EBU 3.75 SH guiding catheter Difficult in wiring of LAD with SION wire due to extensive dissection flap all along the LADWe tried the straw technique with finecross and try to wire the true lumen with XTA wire but failed after prolonged attempt IV morphine and nitrocine were given SION wire was remained in true lumen, and we used the Terumo short tip IVUS for guidance, finally able to pass the XTA wire to D1 IVUS able pass to D1 and IVUS repeated showed wire in true lumen but large haematoma at pLAD D1 to pLAD was predilate with 2.0/15 balloon SION and then XTA were used and able to pass to dLAD and confirmed with the short tip IVUS dLAD was stented with 2.25/26 pLAD was treated with 3.0/15 cutting balloon and then stented with 2.75/38 and post dilate with 4.0 NC balloon unable to wire the very distal LAD and procedure stopped due to already 4-5 hour procedure, patient symptom much relieved and haemodynamic stable
However, CK was found serially normal !!Symptom recurred on and off and BP fluctuate CT Aortogram was arranged and confirmed Type A Intramural haematoma and Type B aortic dissection. Patient transferred to CTSU, but conservative treatment adopted in view of recent PCI.Patient recovered well and discharge uneventfully Recent follow up was well and await follow up CT coro and aortogram.
CTL Coro 3.mov
CTL post PCI 2.mov

However, CK was found serially normal !!Symptom recurred on and off and BP fluctuate CT Aortogram was arranged and confirmed Type A Intramural haematoma and Type B aortic dissection. Patient transferred to CTSU, but conservative treatment adopted in view of recent PCI.Patient recovered well and discharge uneventfully Recent follow up was well and await follow up CT coro and aortogram.
Case Summary
A case of double dissection involving coronary and aortic dissection in the same patient. Vascular dissection is a Demon to interventional cardiology. The coronary dissection likely to be a chronic one and we spend on our focus to treat the coronary Demon. But the real Demon is in the aorta, which account for patient's acute event. We need to stay open-minded and think of other possibilities in case of condition change.