CASE20250805_001
Chronic Total Occlusion With Stent Dislodgement: Successful Retrieval and Revascularization in a Complex Coronary Intervention
By Tzyy-Jer Hsu
Presenter
Tzyy-Jer Hsu
Authors
Tzyy-Jer Hsu1
Affiliation
Chang Gung Memorial Hospital Linkou Branch, Taiwan1
View Study Report
CASE20250805_001
Complication Management - Complication Management
Chronic Total Occlusion With Stent Dislodgement: Successful Retrieval and Revascularization in a Complex Coronary Intervention
Tzyy-Jer Hsu1
Chang Gung Memorial Hospital Linkou Branch, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
Our patient is a 79-year-old female has the history of 1.Left internal carotid artery stenosis s/p stenting on 2020/06,mRS=0, 2.Hypertension, 3.Type 2 Diabetes mellitus and 4.Dyslipidemia whopresented with unstable angina. Initially, she experienced typical anginasymptoms and was under outpatient follow-up. However, her symptoms recentlyworsened, prompting a visit to the emergency department.
Relevant Test Results Prior to Catheterization
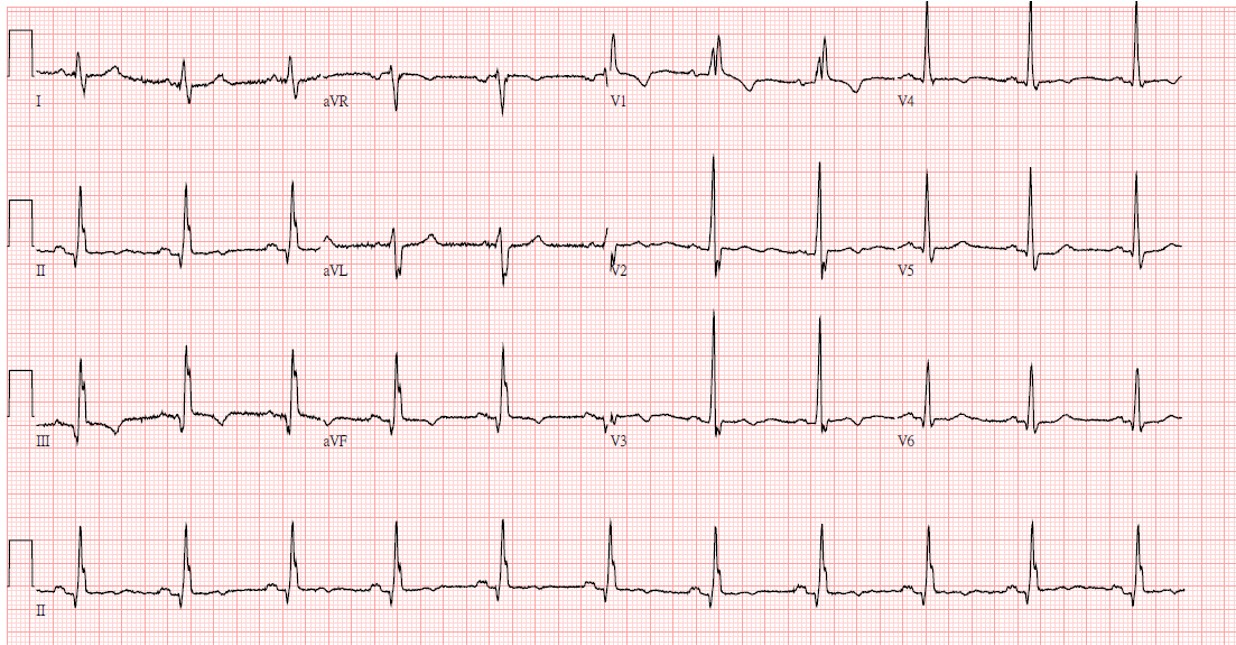
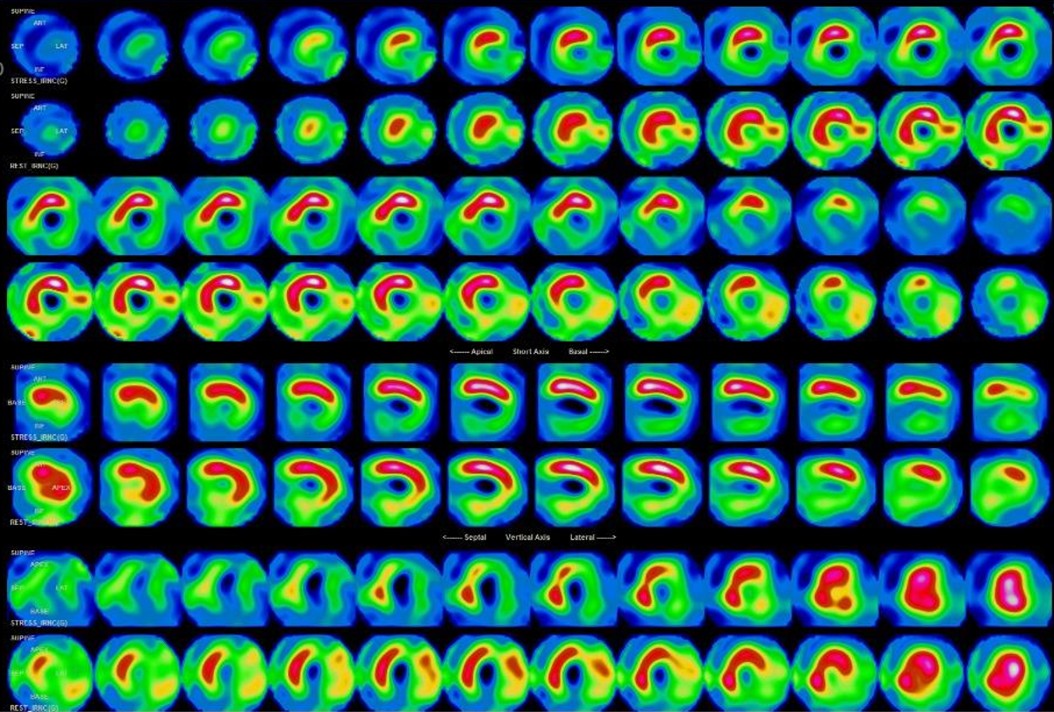
Previously,during outpatient follow-up, she underwent a myocardial perfusion scan, whichrevealed RCA infarction. In the LAD and LCx territories, the findings indicatedmixed ischemia and infarction. An echocardiogram showed a borderline LVEF of49%
Relevant Catheterization Findings
- RCA: Total occlusion with bridging collateral channels to the middle RCA. LAD: Chronic total occlusion at the middle LAD segment with CC2 collateral from the ipsilateral diagonal branch to the distal LAD. Additionally, there was 68% stenosis at the diagonal 1 branch. LCx: Chronic total occlusion at the middle LCxsegment with collateral from the diagonal branch to the OM.
Interventional Management
Procedural Step
Highlights: "CTO intervention of the LAD with retrograde rescue of a major diagonal branch, complicated by stent dislodgement during PCI." We attempted CTO intervention for the LAD by Fielder XT-A wire, and Caravel microcatheter. Angiography showed worsening stenosis at the ostium of a major diagonal branch then A 2.0 mm balloon dilatation was performed. We switched to a retrograde approach via the diagonal branch using a Sion wire and Caravel microcatheter, successfully crossing collaterals and puncturing the distal CTO cap with a Gaia Second wire. Antegrade wiring was achieved and a 2.75 × 38 mm stent was deployed with good LAD results. However, the diagonal branch still had significant dissection, though TIMI 3 flow was preserved. We then proceeded to treat the LCx CTO. Meanwhile, the diagonal branch worsened with slower flow. With dual guiding catheters, we wired both LAD and diagonal. Retraction also failed, as the stent could not be pulled back into the guiding catheter, likely due to poor coaxial alignment damaging the proximal edge. The stent was moved to the femoral region, where balloon-assisted retrieval was unsuccessful. A Snare Technique finally allowed stent removal, but diagonal wires were lost. A retrograde approach from the LAD into the diagonal achieved externalization with TAP for diagnoal lesion
 Rescue D1 retrograde.AVI
Rescue D1 retrograde.AVI
Snare Technique.AVI
Case Summary
CTO intervention of the LAD with retrograde rescue of a major diagonal branch was complicated by stent dislodgement. Two key lessons were learned. First, angiography should include careful assessment of all vessels, not only the target, especially when unstable lesions are present. Diagonal ostium dissection highlighted the need for early recognition, retrograde rescue, and sometimes a two-stent strategy for significant side branches. Second, total stent loss is a critical complication with the guidewire in situ. Prompt recognition and proper retrieval—snaring for proximal loss or multiwire for proximal to mid-vessel—are essential to reduce risk and achieve procedural success.