CASE20250809_002
Long Lesions to Go - A Complex TVD
By Chun Lin Raymond Cheung
Presenter
Chun Lin Raymond Cheung
Authors
Chun Lin Raymond Cheung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1
View Study Report
CASE20250809_002
Complex PCI - Multi-Vessel Disease
Long Lesions to Go - A Complex TVD
Chun Lin Raymond Cheung1
Tuen Mun Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
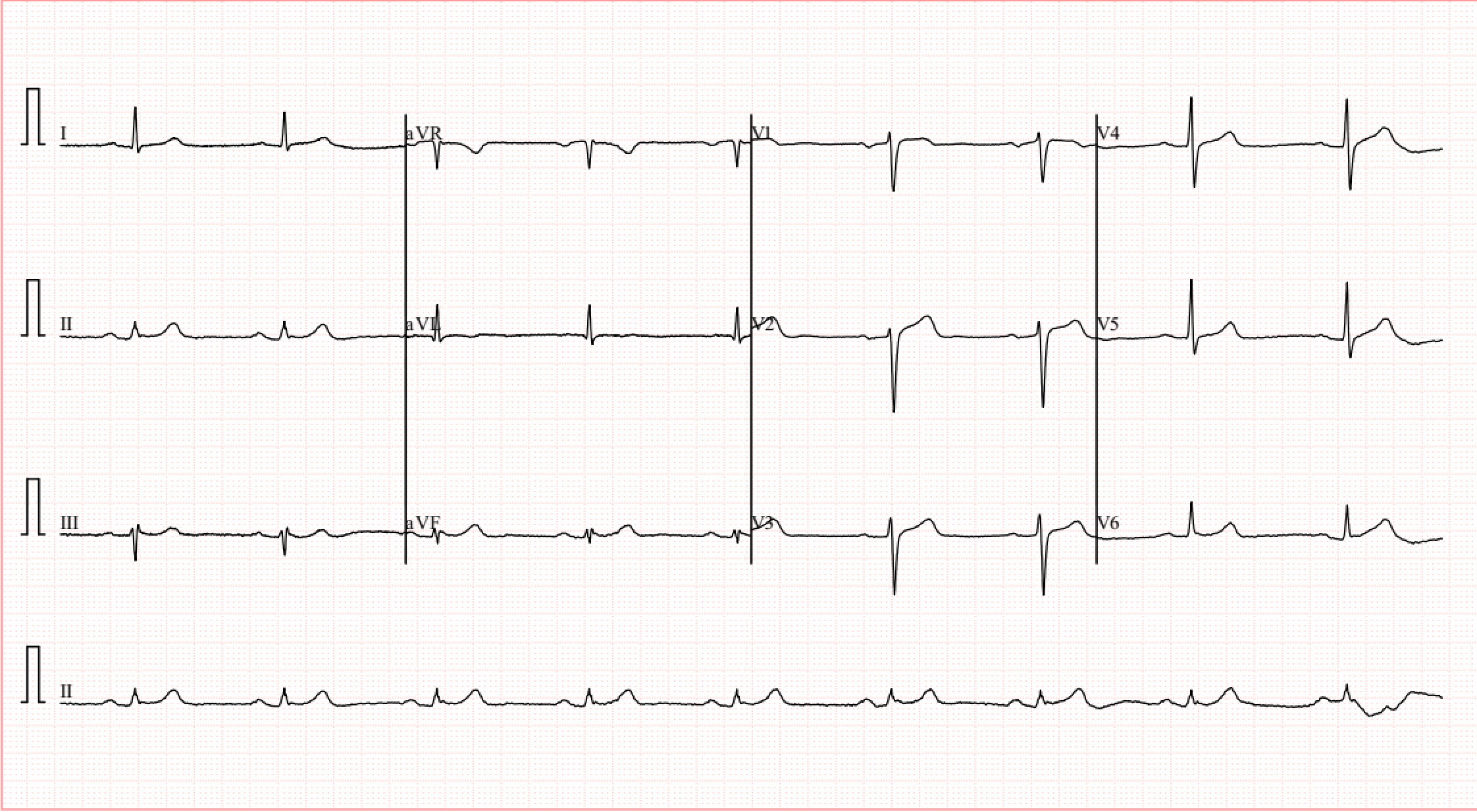
Mr L is a 66 year old man with history of hypertension. hyperlipidemia and diabetes. He had PCI done in 2008 with DES x2 implanted at p-mLAD.He complained of on and off chest discomfort.CTCA done showed in-stent restenosis at LAD and significant stenosis also at LCx and RCA.He was not keen for CABG and opted for PCI.ECG showed sinus rhythm with no acute ST changes.
Relevant Test Results Prior to Catheterization
Blood tests were unremarkable. Troponin levels were not elevated.Echo showed Mildly impaired LV systolic function with LVEF 48% and Global hypokinesia. Heart valves are grossly unremarkable.
 4ch.avi
4ch.avi
sax.avi
lax.avi
Relevant Catheterization Findings
Coronary angiogramCalcified vesselsLM: dLM 20%LAD: p-mLAD 70-80% diffuse ISR followed by CTO right after D1 bifurcationLCx: mLCX 80%, dLCX 80%, pOM 90%RCA: dominant, pRCA 70%, mRCA ~90% with haziness, ostial PL 70%, mid-PDA subtotal occlusion (TIMI 3 flow); retrograde to LADConclusion: further progression of TVD with LAD CTO
lad.avi
lcx.avi
rca.avi
Interventional Management
Procedural Step
Access: RFA & LFAPlan: PCI to RCA, LCx & LAD
RCA engaged with JR4mRCA dilated with 3,0 balloonXience 3.0/28 stent deployed Stent dilated with 3.5 balloon PDA dilated with 2.75/15DEB to PDA done with Pantera LUX 2.5/25OCT showed satisfactory result
LM engaged with EBU 3.5 7FDual injection showed short segment LAD ISR CTOOM1 dilated with 2.0 balloon, DEB done with Pantera LUX 2.0/20OM2 dilated with 2.0 balloon, DEB done with Pantera LUX 2.0/30pLCx dilated with 3.0 balloon, Xience 3.5/15 stent deployed Stent dilated with 3.5 balloon
NS Runthrough and corsair Pro delivered at pLAD. LAD dilated with 2.0 balloon CTO cross with Gaia 2. True lumen confirmed with contralateral injection. Wire switched to NS Runthrough.OCT showed 2 old stents did not overlap with gap in between Calcium nodule noted at CTO site CTO lesion dilated with 3.0 balloon & 3.0 shockwave m-dLAD dilated with 2.0 and 2.5 balloon
OCT showed dissected calcium nodulePlan DEB due to underexpansion from protruding calcium nodule dLAD stented with Xience 2.5/38Stent dilated with 2.5 balloon DEB to old LAD stents with Magic Touch 3.0/35
Xience 3.5/23 stent deployed at LM-pLAD Stent dilated with 4.0 and 3.5 balloon OCT showed satisfactory result
Conclusion: Successful PTCA/S to LM-pLAD (DESx1), p-mLAD (DEB), dLAD (DESx1), pLCx (DESx1), OM1 (DEB), OM2 (DEB), mRCA (DESx1) & PDA (DEB).
stent not overlap.avi
lad stented.avi
rca stented.avi
RCA engaged with JR4mRCA dilated with 3,0 balloonXience 3.0/28 stent deployed Stent dilated with 3.5 balloon PDA dilated with 2.75/15DEB to PDA done with Pantera LUX 2.5/25OCT showed satisfactory result
LM engaged with EBU 3.5 7FDual injection showed short segment LAD ISR CTOOM1 dilated with 2.0 balloon, DEB done with Pantera LUX 2.0/20OM2 dilated with 2.0 balloon, DEB done with Pantera LUX 2.0/30pLCx dilated with 3.0 balloon, Xience 3.5/15 stent deployed Stent dilated with 3.5 balloon
NS Runthrough and corsair Pro delivered at pLAD. LAD dilated with 2.0 balloon CTO cross with Gaia 2. True lumen confirmed with contralateral injection. Wire switched to NS Runthrough.OCT showed 2 old stents did not overlap with gap in between Calcium nodule noted at CTO site CTO lesion dilated with 3.0 balloon & 3.0 shockwave m-dLAD dilated with 2.0 and 2.5 balloon
OCT showed dissected calcium nodulePlan DEB due to underexpansion from protruding calcium nodule dLAD stented with Xience 2.5/38Stent dilated with 2.5 balloon DEB to old LAD stents with Magic Touch 3.0/35
Xience 3.5/23 stent deployed at LM-pLAD Stent dilated with 4.0 and 3.5 balloon OCT showed satisfactory result
Conclusion: Successful PTCA/S to LM-pLAD (DESx1), p-mLAD (DEB), dLAD (DESx1), pLCx (DESx1), OM1 (DEB), OM2 (DEB), mRCA (DESx1) & PDA (DEB).
Case Summary
This case illustrates a challenging scenario involving LM + TVD & LAD ISR CTO with diffuse long calcified lesions.Cross ingthe CTO lesion was difficult due to the calcified lesion, with the guidance of contralateral injection for distal track. OCT was used to characterize the CTO which was due to protruding calcium nodule, and could help guide the strategy for treating the lesion.DEB was performed for side branch lesion to avoid bifurcation stenting.DEB was also performed for the calcified lesion where stents may not fully expand if deployed. Complete revascularization was achieved with different strategies involved.