CASE20250811_001
Collateral Conquest: Retrograde CTO Recanalization Via Septal Highways With Precision Microcatheter-Guided Stent Deployment in a Post CABG Patient
By Agnes Dinar Putrinarita, Arwin Saleh Mangkuanom, Amir Aziz Alkatiri, Nanda Iryuza, Doni Firman
Presenter
Agnes Dinar Putrinarita
Authors
Agnes Dinar Putrinarita1, Arwin Saleh Mangkuanom1, Amir Aziz Alkatiri1, Nanda Iryuza1, Doni Firman1
Affiliation
National Cardiovascular Centre Harapan Kita, Indonesia1
View Study Report
CASE20250811_001
Complex PCI - CTO
Collateral Conquest: Retrograde CTO Recanalization Via Septal Highways With Precision Microcatheter-Guided Stent Deployment in a Post CABG Patient
Agnes Dinar Putrinarita1, Arwin Saleh Mangkuanom1, Amir Aziz Alkatiri1, Nanda Iryuza1, Doni Firman1
National Cardiovascular Centre Harapan Kita, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 50-year-old male with exertional chest pain and history of triple-grafts CABG performed one year prior presented with complex coronary artery disease and chronic kidney disease stage 3a, alongside hypertension, dyslipidaemia, and a family history of coronary artery disease. Physical examination was unremarkable.
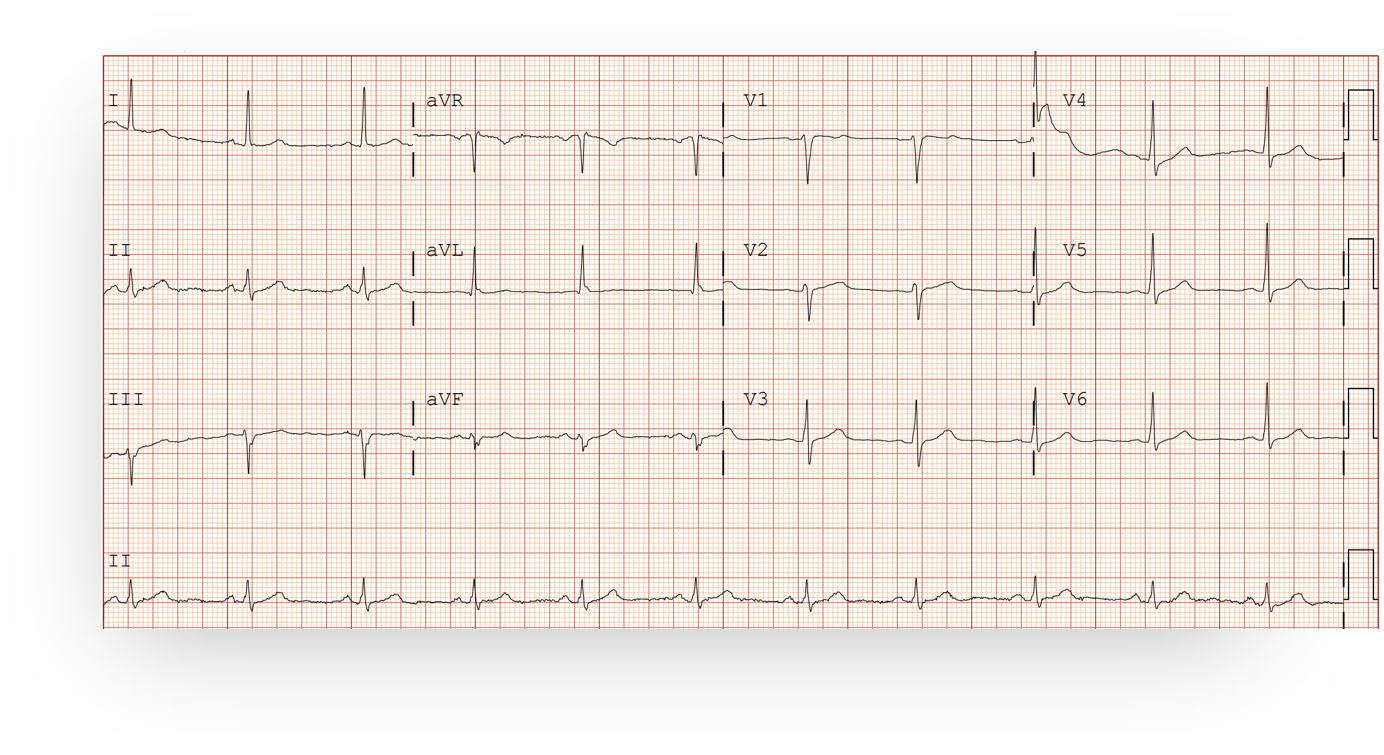
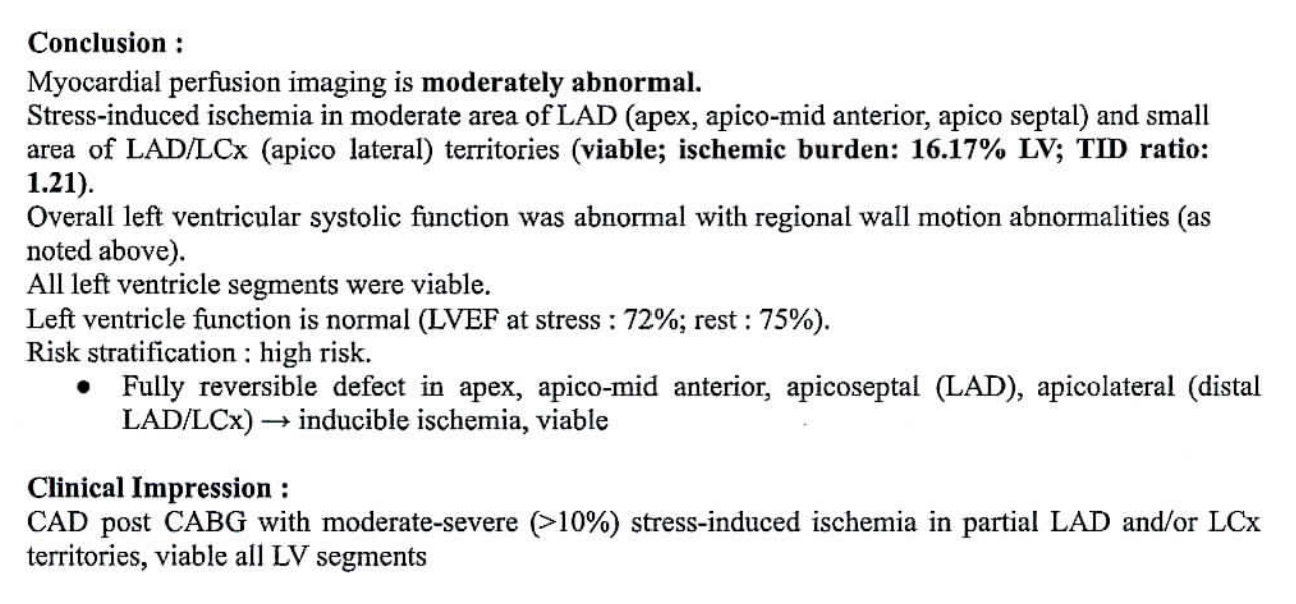
Relevant Test Results Prior to Catheterization
ECG was normal. Myocardial perfusion imaging revealed severe (>10%) stress-induced ischemia in partial LAD and/or LCx territories, with all LV segments remaining viable. Resting and stress LV ejection fraction was preserved.
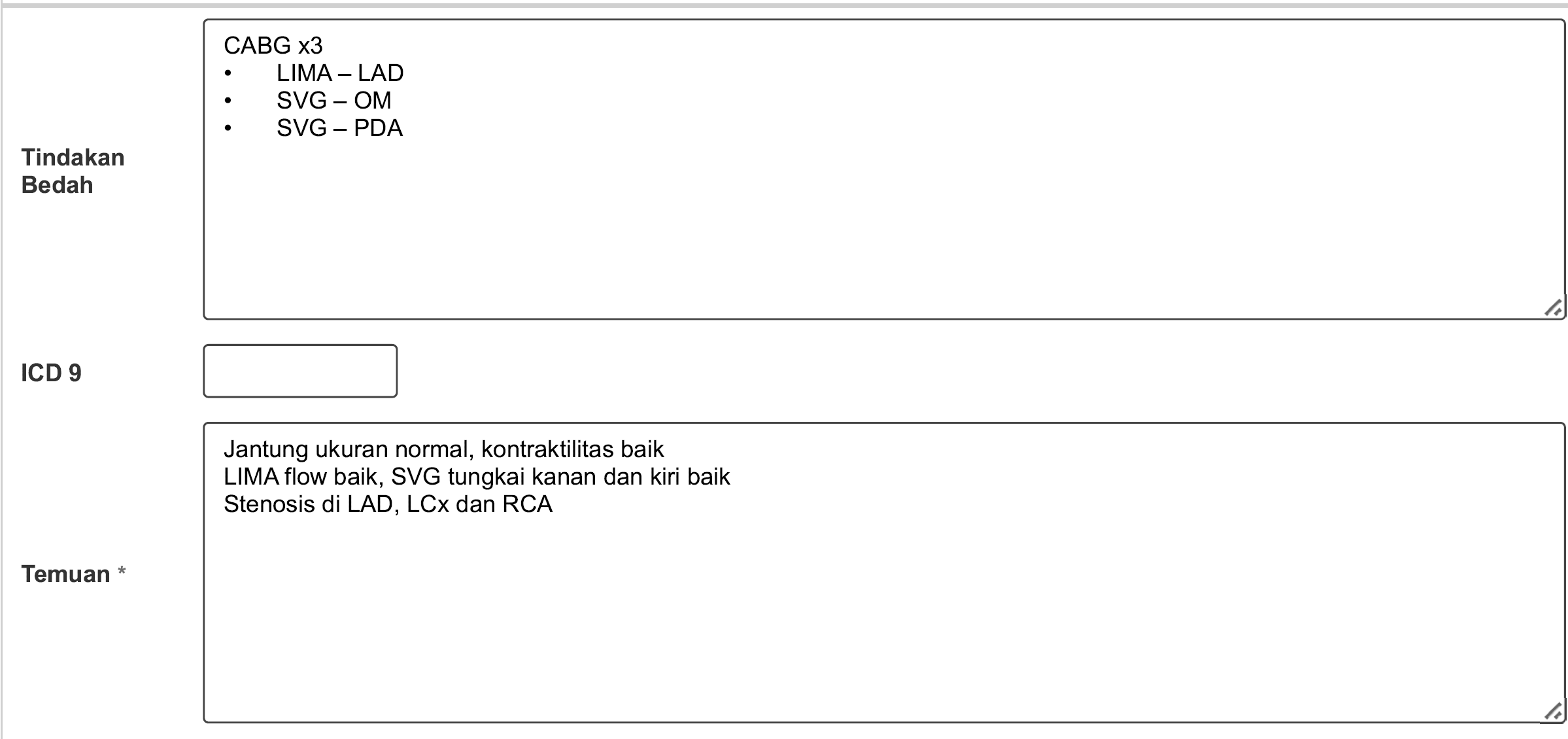
Relevant Catheterization Findings
Coronary angiography revealed proximal LMCA chronic subtotal occlusion with non-visualized LAD and LCx. Native RCA showed diffuse disease with severe distal stenosis. Graft study demonstrated failed LIMA-LAD, patent SVG-OM and SVG-PDA. Rentrop III septal collaterals from PDA via SVG injection provided collateral flow to the left system.
 Gabungan CAG Mr AM.mp4
Gabungan CAG Mr AM.mp4
Interventional Management
Procedural Step
Initial antegrade wiring with NS Floppy then Fielder XT-A backed by Finecross microcatheter successfully crossed into distal LCx territory. Due to ambiguous proximal cap anatomy, retrograde PCI approach was chosen via septal collaterals from RCA using Suoh 03 guidewire to reach distal LAD, with Fielder XT-A successfully crossing the CTO body. Following successful RG3 wire externalization and multiple high-pressure pre-dilatations using NC and scoring balloons, microcatheter tip injection was utilized to enhance precision for ostial left main stent positioning. A DES 3.5×38mm was deployed from proximal LAD extending to ostial left main with optimal positioning confirmed by microcatheter-guided contrast injection. Post-dilation with NC 4.0mm balloon ensured optimal stent apposition and expansion. Additional stenting with 2.5×38mm DES was performed in mid-proximal LAD segment, followed by final optimization using NC 3.5mm balloon post-dilation, achieving excellent angiographic and procedural results under IVUS guidance for optimal stent deployment confirmation. Final angiographic evaluation showed TIMI 3 flow restoration in LM-LAD with no dissection or perforation. Patient was hemodynamically stable, and no immediate complications were reported. The patient is currently symptom-free and maintains regular clinic visits.
2. Septal surfing using Suoh 03.mp4
1. Collateral injection from micro RCA.mp4
Ostial LM stenting guided by microcatheter.mp4
Case Summary
Successful retrograde PCI via septal collaterals achieved excellent outcomes in this complex CTO case with failed surgical grafts. Precise septal collateral selection and microcatheter-guided ostial stent placement were essential for procedural success. This demonstrates that complex CTO intervention can be safely performed in high-risk patients with CKD and prior cardiac surgery through meticulous technique and IVUS guidance. The patient remains asymptomatic with preserved ventricular function, highlighting the clinical benefit of successful complex PCI in selected patients with viable myocardium