CASE20250814_002
A Challenging Case of Complex CTO PCI of the LAD via Right Distal Radial Access in Rajavithi Hospital
By Sajja Jangjit, Wittawat Wattanasiriporn
Presenter
Sajja Jangjit
Authors
Sajja Jangjit1, Wittawat Wattanasiriporn1
Affiliation
Rajavithi Hospital, Thailand1
View Study Report
CASE20250814_002
Complex PCI - CTO
A Challenging Case of Complex CTO PCI of the LAD via Right Distal Radial Access in Rajavithi Hospital
Sajja Jangjit1, Wittawat Wattanasiriporn1
Rajavithi Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
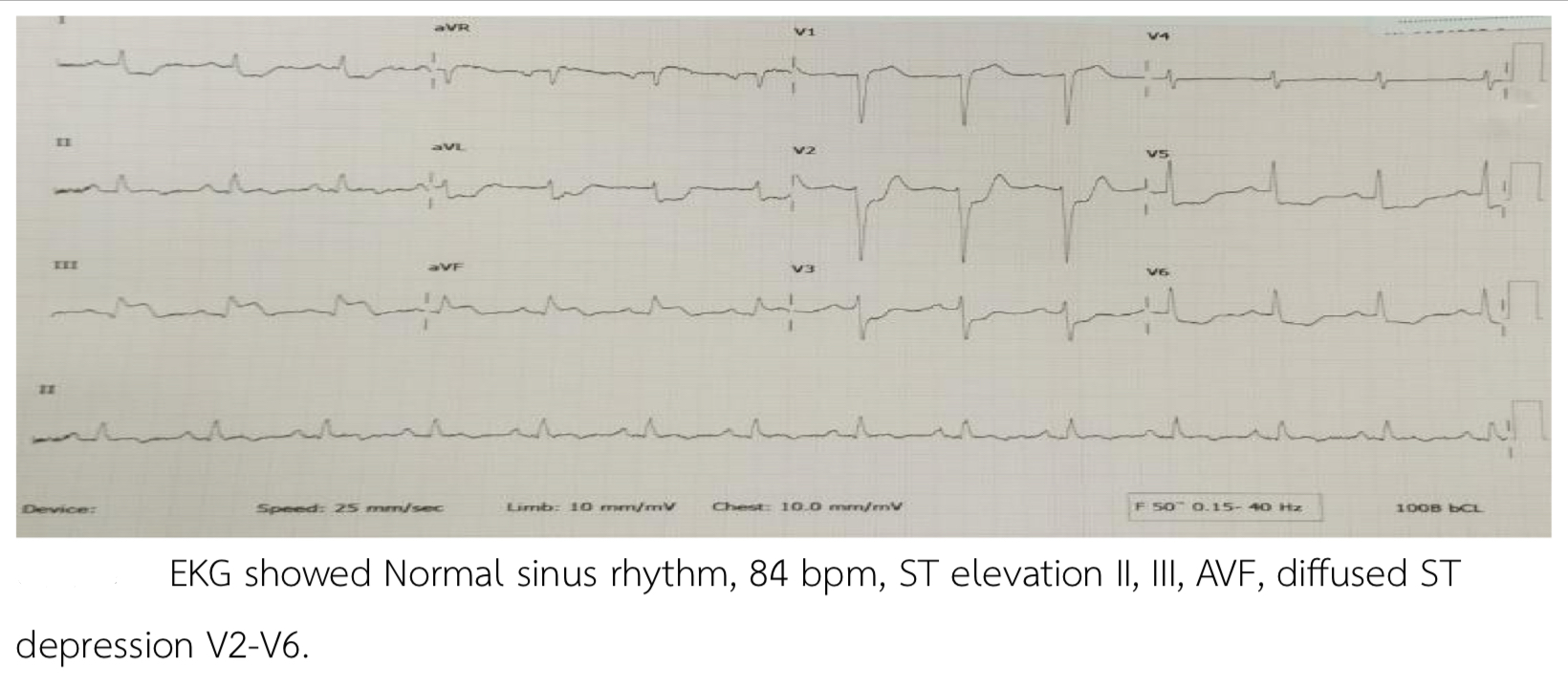
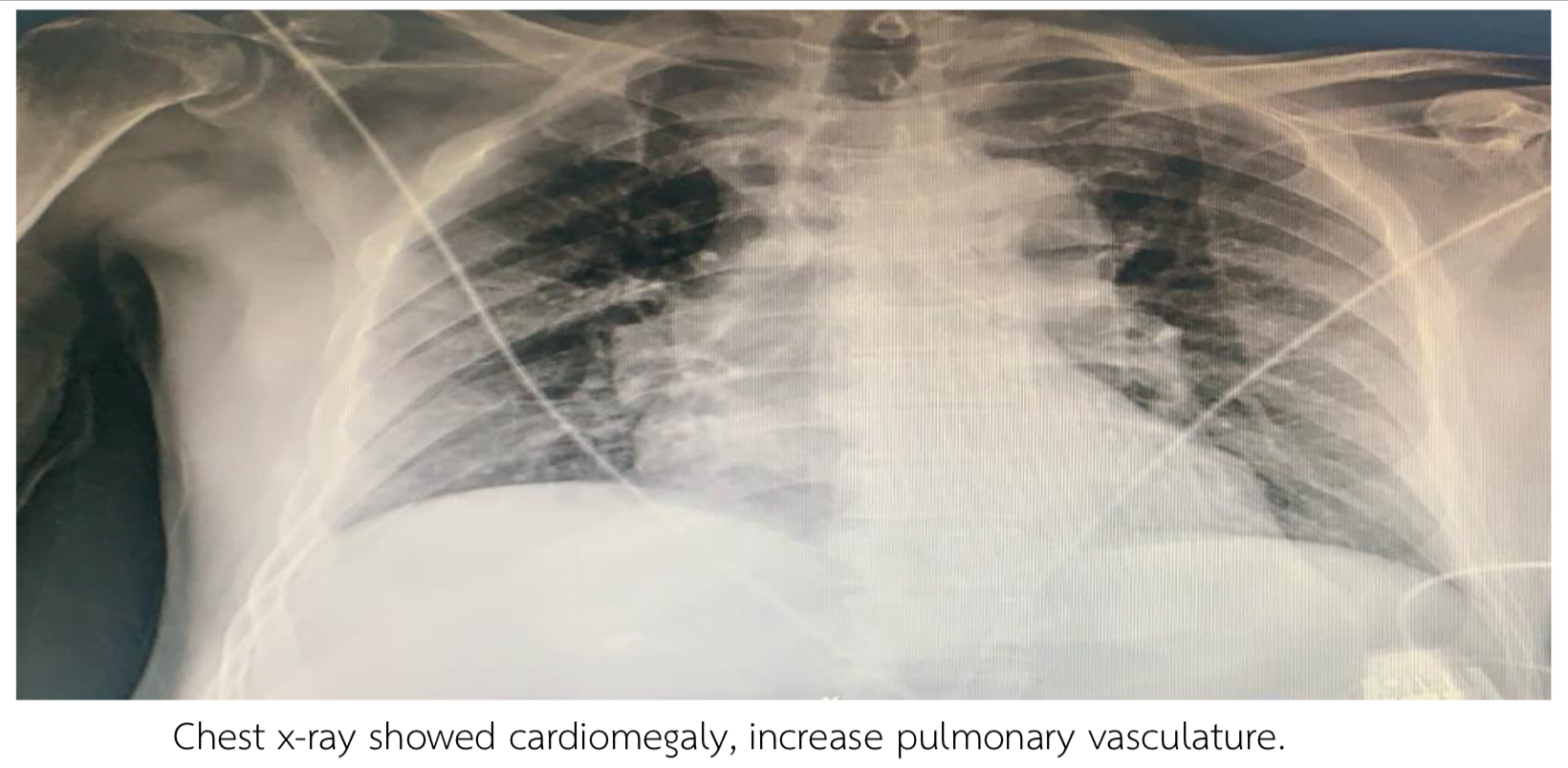
Thai male 69 years, Risk Hypertension, Dyslipidemia presented with chest pain 2 hours prior to admission. Blood pressure 104/62 mmHg Heart rate 76 bpm. Heart regular, fine crepitation both lower lungs. EKG showed Normal sinus rhythm, 84 bpm, ST elevation II, III, AVF, diffused ST depression V2-V6. Echocardiogram showed LVEF 42%, Global wall Hypokinesia, no significant valvular heart disease. Troponin T was positive 10,400 pg/ml. Chest x-ray showed cardiomegaly, increase pulmonary vasculature
Relevant Test Results Prior to Catheterization
EKG showed Normal sinus rhythm, 84 bpm, ST elevation II, III, AVF, diffused ST depression V2-V6. Echocardiogram showed LVEF 42%, Global wall Hypokinesia, no significant valvular heart disease. Troponin T was positive 10,400 pg/ml. Chest x-ray showed cardiomegaly, increase pulmonary vasculature.
Relevant Catheterization Findings
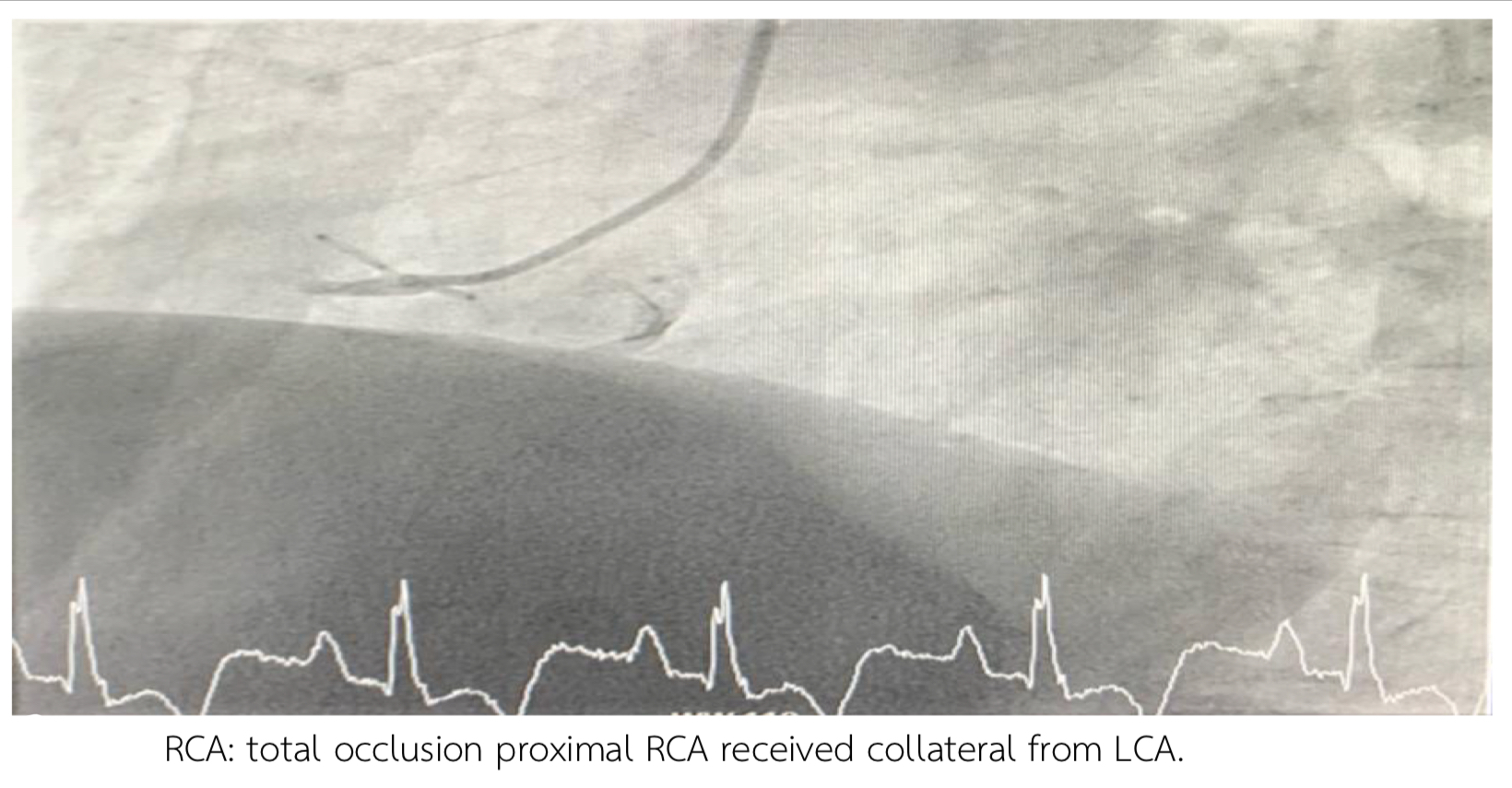
Access: Right radial via 6Fr sheath.- LM: non significant stenosis- LAD: Subtotal occlusion mid-LAD, CTO mid to distal LAD.- LCx: CTO mid-LCx with collateral from OM1.- RCA: Total occlusion proximal RCA with collateral from LCA.

Interventional Management
Procedural Step
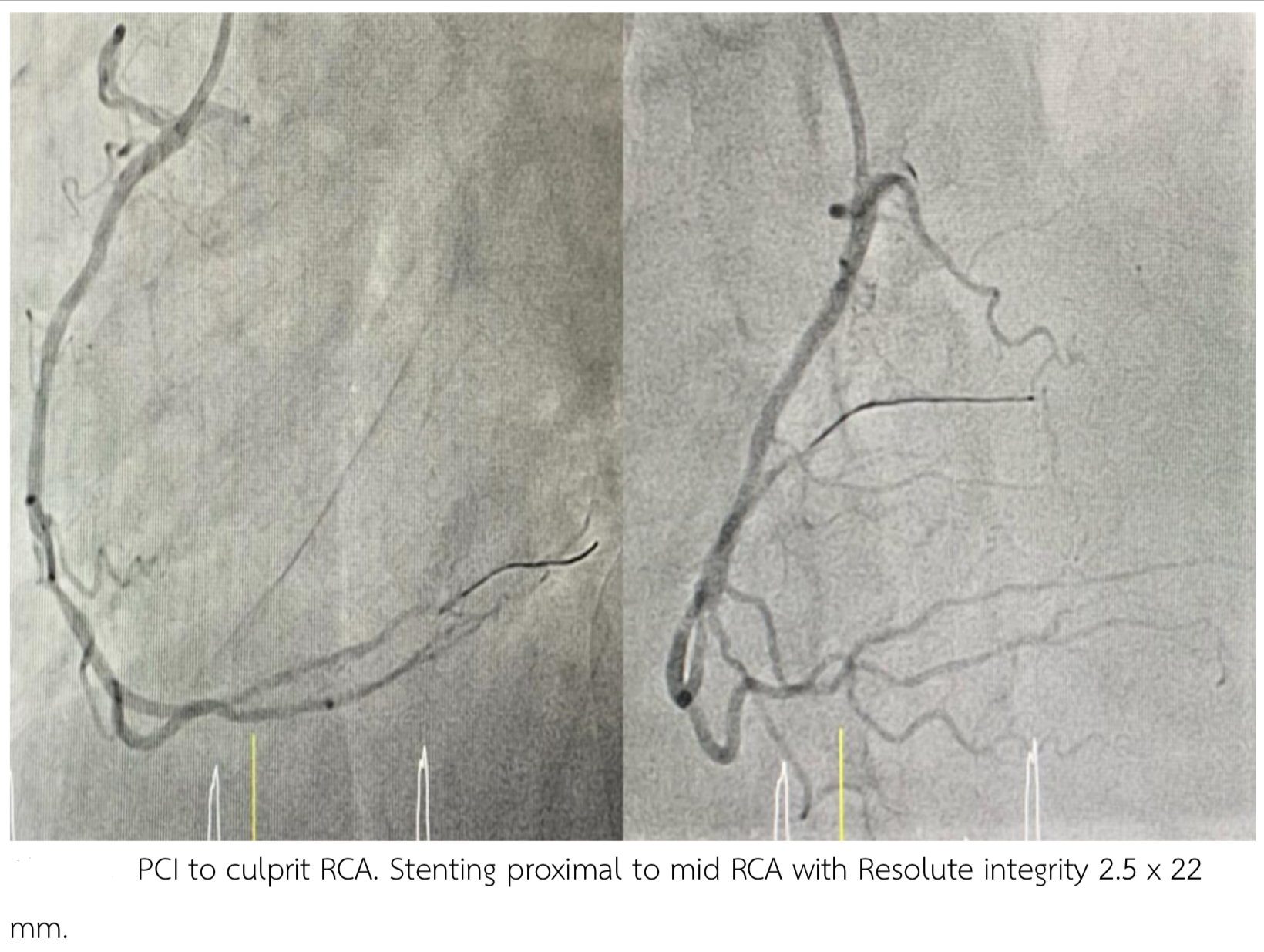
PCI to culprit RCA:Access right radial.Guiding Catheter: 5 Fr Ikari guiding catheterStenting proximal to mid RCA with Resolute integrity 2.5 x 22 mm upto 12 atm.
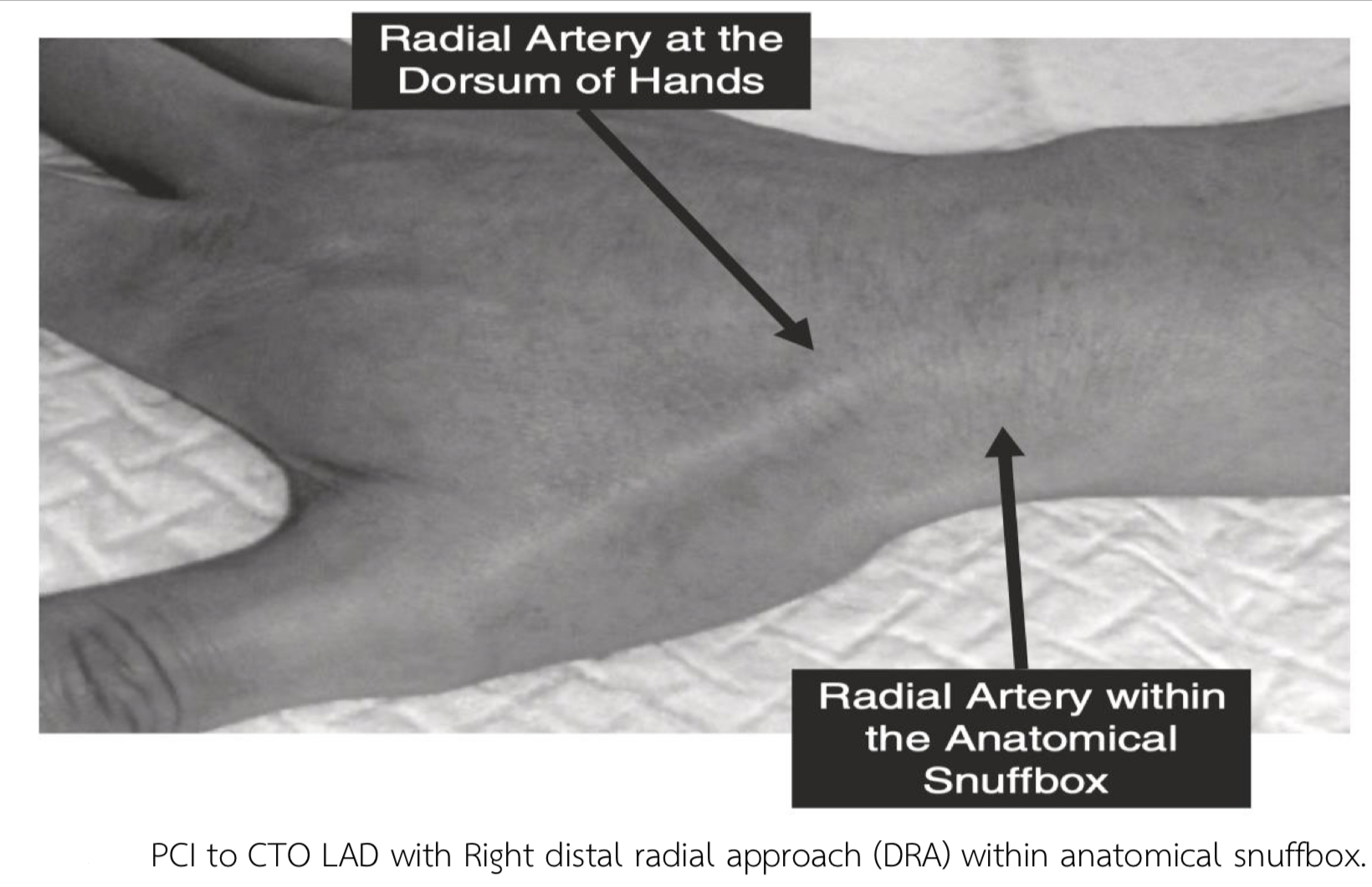
The patient still had chest pain then stage PCI to CTO LAD with Right distal radial approach (DRA).
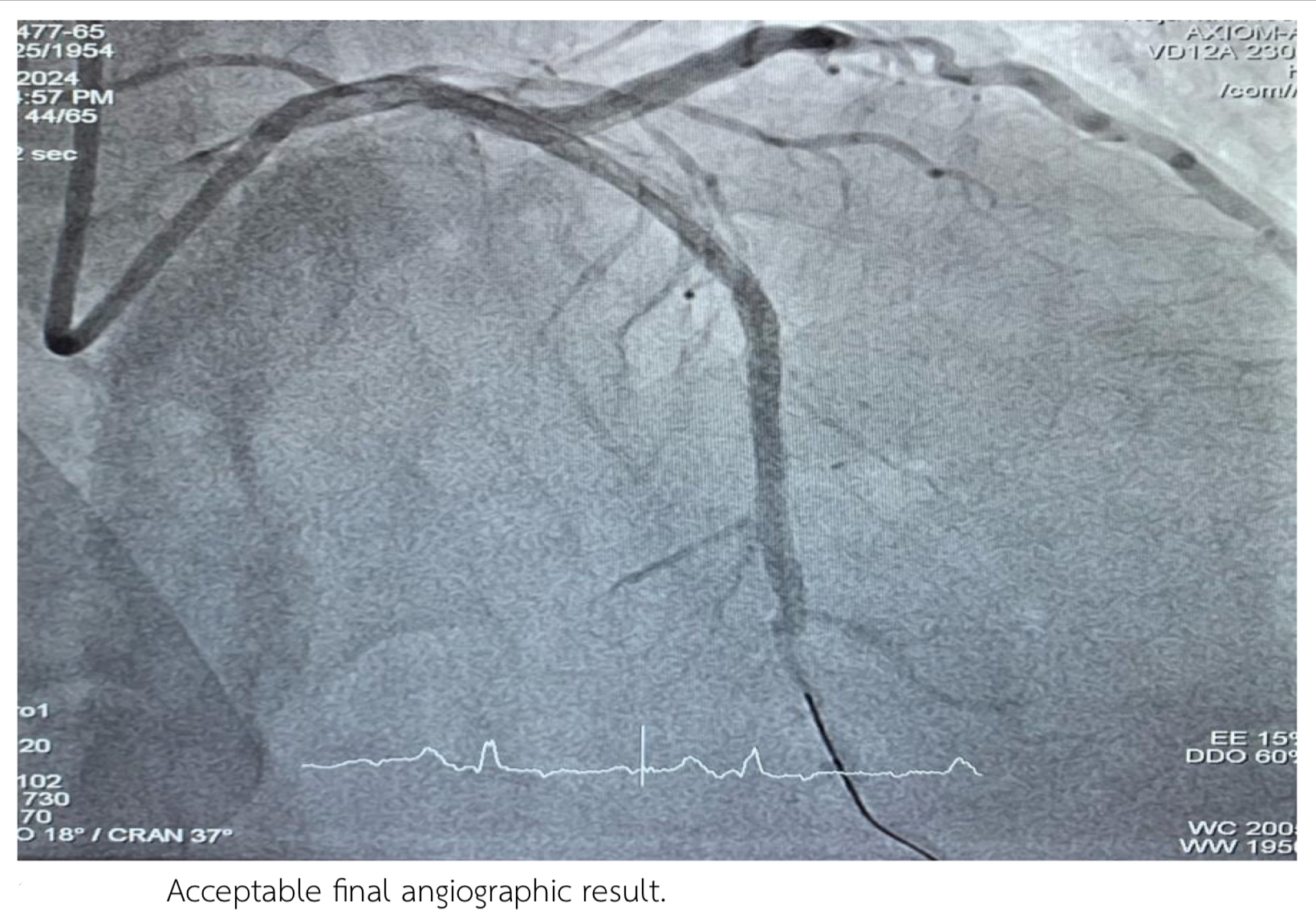
Staged PCI to CTO LAD:Access right distal radial access (DRA) in the anatomical snuffbox.Guiding Catheter: 5 Fr Ikari guiding catheterSion with finecross pass to LAD then change to Fielder XT pass through CTO LAD.Tip injection revealed true lumen wiring .Semi-compliant balloon 2.0 x 15 mm inflated p-dLAD upto 14 atm.Xience ProA 2.5 x 38 mm deployed mid to distal LAD upto 12 atm. Resolute integrity 2.75 x 30 mm deployed proximal to mid LAD upto 12 atm. Acceptable angiographic result.

The patient still had chest pain then stage PCI to CTO LAD with Right distal radial approach (DRA).
Staged PCI to CTO LAD:Access right distal radial access (DRA) in the anatomical snuffbox.Guiding Catheter: 5 Fr Ikari guiding catheterSion with finecross pass to LAD then change to Fielder XT pass through CTO LAD.Tip injection revealed true lumen wiring .Semi-compliant balloon 2.0 x 15 mm inflated p-dLAD upto 14 atm.Xience ProA 2.5 x 38 mm deployed mid to distal LAD upto 12 atm. Resolute integrity 2.75 x 30 mm deployed proximal to mid LAD upto 12 atm. Acceptable angiographic result.
Case Summary
The distal radial approach (DRA) is a feasible and safe alterative for complex PCI.Using a 5 Fr guiding cather is effective for complex lesion like CTOs and reduces vascular complications.This case report demonstrates the a complex CTO LAD can be successfully treated with a minimalist approach using right DRA and a 5 Fr Ikari guiding catheter.percutaneous coronary intervention (PCI) for chronic total occlusion (CTO) using a 5 Fr radial Ikari guide catheter can be successful in selected cases.