CASE20250815_002
From Jailed to Saved: Bailout LM PCI in Cardiogenic Shock
By Subin Lim
Presenter
Subin Lim
Authors
Subin Lim1
Affiliation
Ewha Womans University Seoul Hospital, Korea (Republic of)1
View Study Report
CASE20250815_002
Complex PCI - Left Main
From Jailed to Saved: Bailout LM PCI in Cardiogenic Shock
Subin Lim1
Ewha Womans University Seoul Hospital, Korea (Republic of)1
Clinical Information
Relevant Clinical History and Physical Exam
A 70-year-old female patient complaining of squeezing chest pain was admitted to the emergency department, shortly after which she collapsed. She regained consciousness and became slightly drowsy while measuring the vital signs, which showed a blood pressure of 65/43 mm Hg and heart rate 82 bpm. After IV fluid and norepinephrine administration, her blood pressure recovered to 90/54 mm Hg.
Relevant Test Results Prior to Catheterization
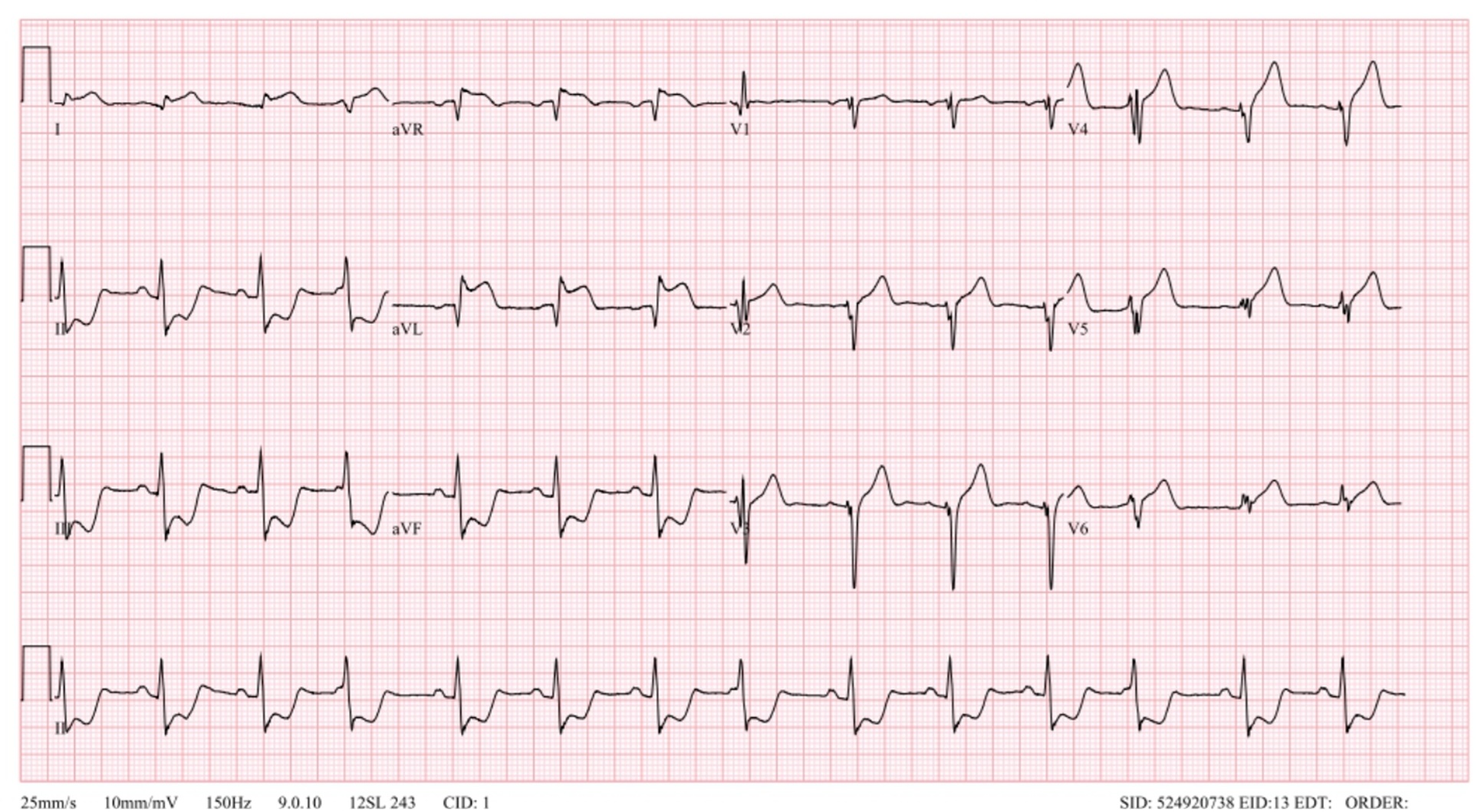
The ECG showed elevation in lead I, aVL and aVR, with diffuse ST depressions in leads II, III and aVF. The cath lab was activated for ST elevation myocardial infarction.
Relevant Catheterization Findings
Baseline angiography showed subtotal occlusion of distal left main vessel, with diffuse 90% stenosis in proximal-midLAD, 90% stenosis in ostial LCX and 80% stenosis in distal RCA.
 01baserca.mp4
01baserca.mp4
02basecau.mp4
03basecra.mp4
Interventional Management
Procedural Step
Using a JL 7-Fr guide, the LAD was wired with a conventional workhorse guidewire. Due to severe angulation and tight stenosis, LCX wiring was difficult, and the patient started to complain of chest pain so LM ballooning was performed. During unsuccessful LCX wiring attempts, the BP began to drop to 86/50 mm Hg. A decision was made to first stent the LM-LAD to improve the LM-LAD blood flow. DES 2.5x30 for pmLAD and DES 3.0x22 for LM-LAD were successfully deployed. Follow-up angiogram showed that the unwired LCX was jailed from the ostium and was no longer visible. At this point, the patient began to crash and we had to intubate.
The distal LM culprit site was underexpanded, so an NC balloon 3.0x9mm was used to post-dilate the stent but the LCX was still jailed. After 30 minutes of unsuccessful wiring, the LCX was wired with an angled microcatheter (Supercross 90°). A 1.5x15 and a 2.5x15 mm balloon were used sequentially to dilate the ostial LCX. LCX flow returned to TIMI 3, and IVUS imaging showed a calcified nodule in proximal LCX and dissection at ostial-proximal LCX. Provisional LCX stenting was decided but the DES could not advance into the LCX. LAD stent anchor balloon was unsuccessful, as were a more distal LAD anchor balloon, a cutting balloon and Guidezilla. Dilation with 3.0-mm NC balloon achieved Guidezilla advancement and stent deployment at LM-LCX. Bifurcation PCI using culotte technique was performed. Final kissing balloon and POT achieved successful LM PCI.
13poststent.mp4
18lcxwiresuccess.mp4
42final.mp4
The distal LM culprit site was underexpanded, so an NC balloon 3.0x9mm was used to post-dilate the stent but the LCX was still jailed. After 30 minutes of unsuccessful wiring, the LCX was wired with an angled microcatheter (Supercross 90°). A 1.5x15 and a 2.5x15 mm balloon were used sequentially to dilate the ostial LCX. LCX flow returned to TIMI 3, and IVUS imaging showed a calcified nodule in proximal LCX and dissection at ostial-proximal LCX. Provisional LCX stenting was decided but the DES could not advance into the LCX. LAD stent anchor balloon was unsuccessful, as were a more distal LAD anchor balloon, a cutting balloon and Guidezilla. Dilation with 3.0-mm NC balloon achieved Guidezilla advancement and stent deployment at LM-LCX. Bifurcation PCI using culotte technique was performed. Final kissing balloon and POT achieved successful LM PCI.
Case Summary
PCI for the LM bifurcation is always challenging, especially in an ACS setting because it is difficult to plan ahead. The LCX is a side branch in the LM bifurcation, but an important one which needs to be saved. During an emergency PCI for the LM bifurcation, priorities must be selected wisely, sometimes with bold and rapid decisions in order to successfully complete the procedure.