CASE20250815_003
Total Makeover of Complex CAD: Rotablator, Cutting Balloon, and Stenting in Undilatable RCA, CTO LCX, and LM-LAD
By Rido Adrianto Sukaton, Amir Aziz Alkatiri, Arwin Saleh Mangkuanom, Nanda Iryuza, Doni Firman
Presenter
Rido Adrianto Sukaton
Authors
Rido Adrianto Sukaton1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Doni Firman1
Affiliation
RSJPD Harapan Kita, Indonesia1
View Study Report
CASE20250815_003
Complex PCI - Multi-Vessel Disease
Total Makeover of Complex CAD: Rotablator, Cutting Balloon, and Stenting in Undilatable RCA, CTO LCX, and LM-LAD
Rido Adrianto Sukaton1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Doni Firman1
RSJPD Harapan Kita, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 56-year-old male presented with angina pectoris during daily activities. Risk factors included hypertension, dyslipidemia, and ex-smoker status. Physical examination findings were within normal limits.
 Screen Recording 2025-08-17 at 08.06.35.mov
Screen Recording 2025-08-17 at 08.06.35.mov
Relevant Test Results Prior to Catheterization
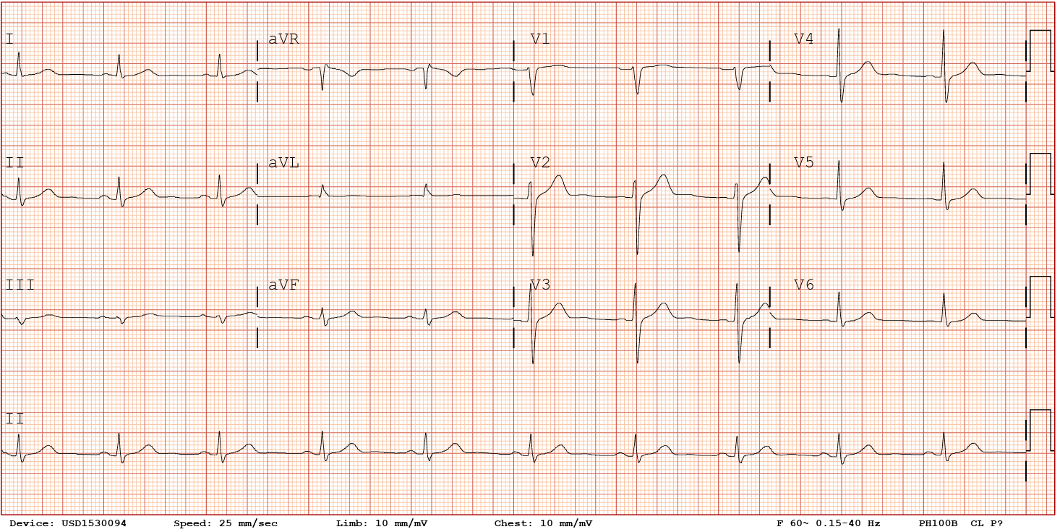
Resting ECG was normal treadmill test showed positive ischemic response with high-risk Duke score. Coronary CTA revealed three-vessel CAD. Angiography showed RCA distal subtotal stenosis, LAD with diffuse calcified subtotal stenosis from ostial–mid, and OM2 proximal CTO. Attempted PCI to RCA failed due to undilatable calcified lesion.
Relevant Catheterization Findings
Dominant RCA with calcification, proximal tubular 70–80% stenosis, distal tubular subtotal stenosis. LM normal. LAD with calcification and diffuse stenosis from ostial–mid, with subtotal stenosis at proximal. LCx proximal tubular 80% stenosis. OM2 diffuse stenosis from ostial–mid with proximal CTO.
Screen Recording 2025-08-15 at 19.24.33.mov
Screen Recording 2025-08-15 at 19.25.21.mov
Interventional Management
Procedural Step
PCI to RCA: Full-dose heparin administered. Runthrough NS Floppy to distal PL; IVUS showed distal RCA 360° calcification. Finecross for exchange to Rota Floppy; aminophylline 240 mg IV. Rotational atherectomy with 1.75 mm burr at 180k rpm, polishing at 150k rpm. IVUS: mid-distal fibro-calcified 90–270°, MLA 3.35 mm², length 30.69 mm. Predilatation with cutting balloon 3.0×15 mm achieved maximal expansion (unlike prior failed attempt). DES 3.5×32 mm deployed, post-dilated with NC 3.5×15 mm high-pressure. IVUS post-stent: MSA 7.85 mm² at distal RCA, TIMI 3.
PCI to LCx: ACT 268, additional heparin given, EBU 3.5/6F. Runthrough NS Floppy with Finecross failed to cross OM2 CTO; escalated to Fielder XT-A, successful. Exchange to Runthrough; predilatation with 2.0×15 mm balloon; IVUS: fibro-calcified 90–270°, MLA 2.26 mm². Another predilatation with NC Scoreflex 2.5×15 mm, DES 2.75×33 mm deployed, post-dilated to 3.0 mm high-pressure. IVUS post-stent: MSA 4.72 mm² at OM, TIMI 3.
PCI to LM–LAD: IVUS showed ostial–mid LAD fibro-calcified 90–270°, MLA 3.42 mm², length 48.5 mm. Predilatation with NC Scoreflex 2.5 mm, escalated to cutting balloon 3.0 mm. DES 3.5×28 mm in mid LAD, overlapped proximally with DES 4.0×28 mm LM–LAD; post-dilated to 4.0 mm high-pressure, POT 5.0 mm. IVUS post-stent: MSA 7.89 mm² at mid LAD, TIMI 3. Procedure completed without complication; total contrast 240 ml, FT 39.4 min, DAP 78.2 Gy·cm².
Screen Recording 2025-08-15 at 19.32.09.mov
Screen Recording 2025-08-15 at 19.35.12.mov
Screen Recording 2025-08-15 at 19.37.02.mov
PCI to LCx: ACT 268, additional heparin given, EBU 3.5/6F. Runthrough NS Floppy with Finecross failed to cross OM2 CTO; escalated to Fielder XT-A, successful. Exchange to Runthrough; predilatation with 2.0×15 mm balloon; IVUS: fibro-calcified 90–270°, MLA 2.26 mm². Another predilatation with NC Scoreflex 2.5×15 mm, DES 2.75×33 mm deployed, post-dilated to 3.0 mm high-pressure. IVUS post-stent: MSA 4.72 mm² at OM, TIMI 3.
PCI to LM–LAD: IVUS showed ostial–mid LAD fibro-calcified 90–270°, MLA 3.42 mm², length 48.5 mm. Predilatation with NC Scoreflex 2.5 mm, escalated to cutting balloon 3.0 mm. DES 3.5×28 mm in mid LAD, overlapped proximally with DES 4.0×28 mm LM–LAD; post-dilated to 4.0 mm high-pressure, POT 5.0 mm. IVUS post-stent: MSA 7.89 mm² at mid LAD, TIMI 3. Procedure completed without complication; total contrast 240 ml, FT 39.4 min, DAP 78.2 Gy·cm².
Case Summary
A patient with three-vessel CAD and prior failed PCI of an undilatable calcified RCA was referred for CABG. Using rotational atherectomy, cutting balloon angioplasty, and IVUS-guided DES implantation, we achieved successful complete revascularization. All target vessels reached optimal stent expansion and TIMI 3 flow without complications.