CASE20250816_001
Myocardial Infarction in a Case With No Left Main Coronary Artery Ostium: A Case Report
By Chinh Duc Nguyen, Cong Dinh Pham, Thi Quynh Huong Tran, Thi Phuong Anh Nguyen
Presenter
Chinh Duc Nguyen
Authors
Chinh Duc Nguyen1, Cong Dinh Pham1, Thi Quynh Huong Tran1, Thi Phuong Anh Nguyen1
Affiliation
Stroke International Services General Hospital, Vietnam1
View Study Report
CASE20250816_001
ACS/AMI - ACS/AMI
Myocardial Infarction in a Case With No Left Main Coronary Artery Ostium: A Case Report
Chinh Duc Nguyen1, Cong Dinh Pham1, Thi Quynh Huong Tran1, Thi Phuong Anh Nguyen1
Stroke International Services General Hospital, Vietnam1
Clinical Information
Relevant Clinical History and Physical Exam
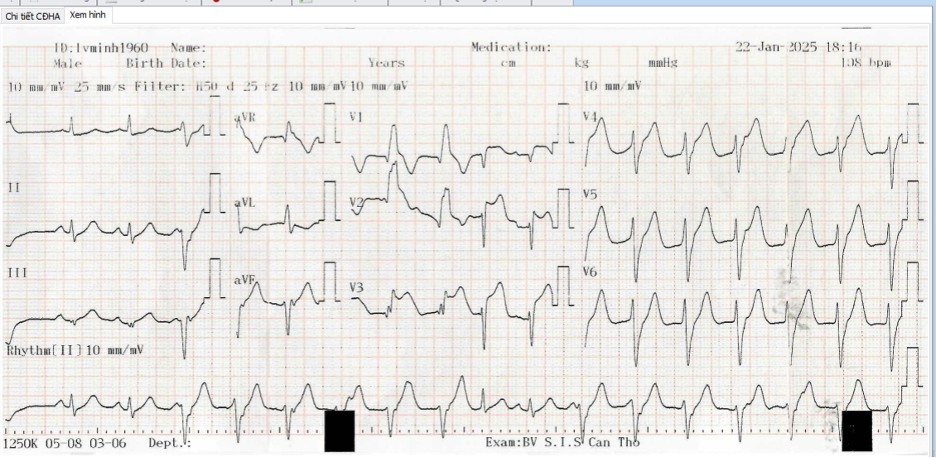
A 66-year-old male was admitted to the Internal Medicine department due to exertion chest pain. 10 hours before admission, he experienced a 10-minute angina episode, which radiated to both shoulders and to the back. Past history included ischemic heart disease. He was dianosed at a local hospital as having anterior myocardial infarction, at hour 1. ECG on admission: sinus rhythm, with non-sustained monomorphic ventricular tachycardia, elevated ST segment in V1-V6.
Relevant Test Results Prior to Catheterization
hs-troponin I was > 50.000 pg/mL, NT-proBNP 1025.1 pg/mL. The transthoracic echocardiogram showed reduced left ventricular function (EF 40 %), with hypokinesis of the apical.
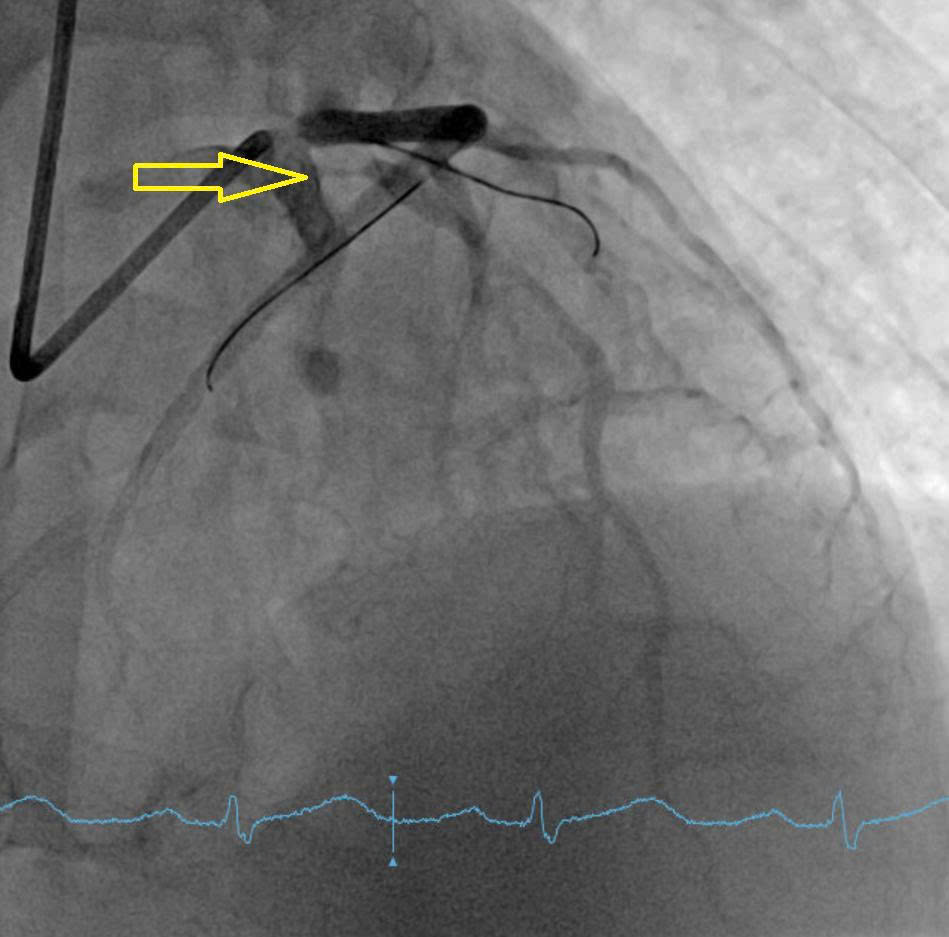
Relevant Catheterization Findings
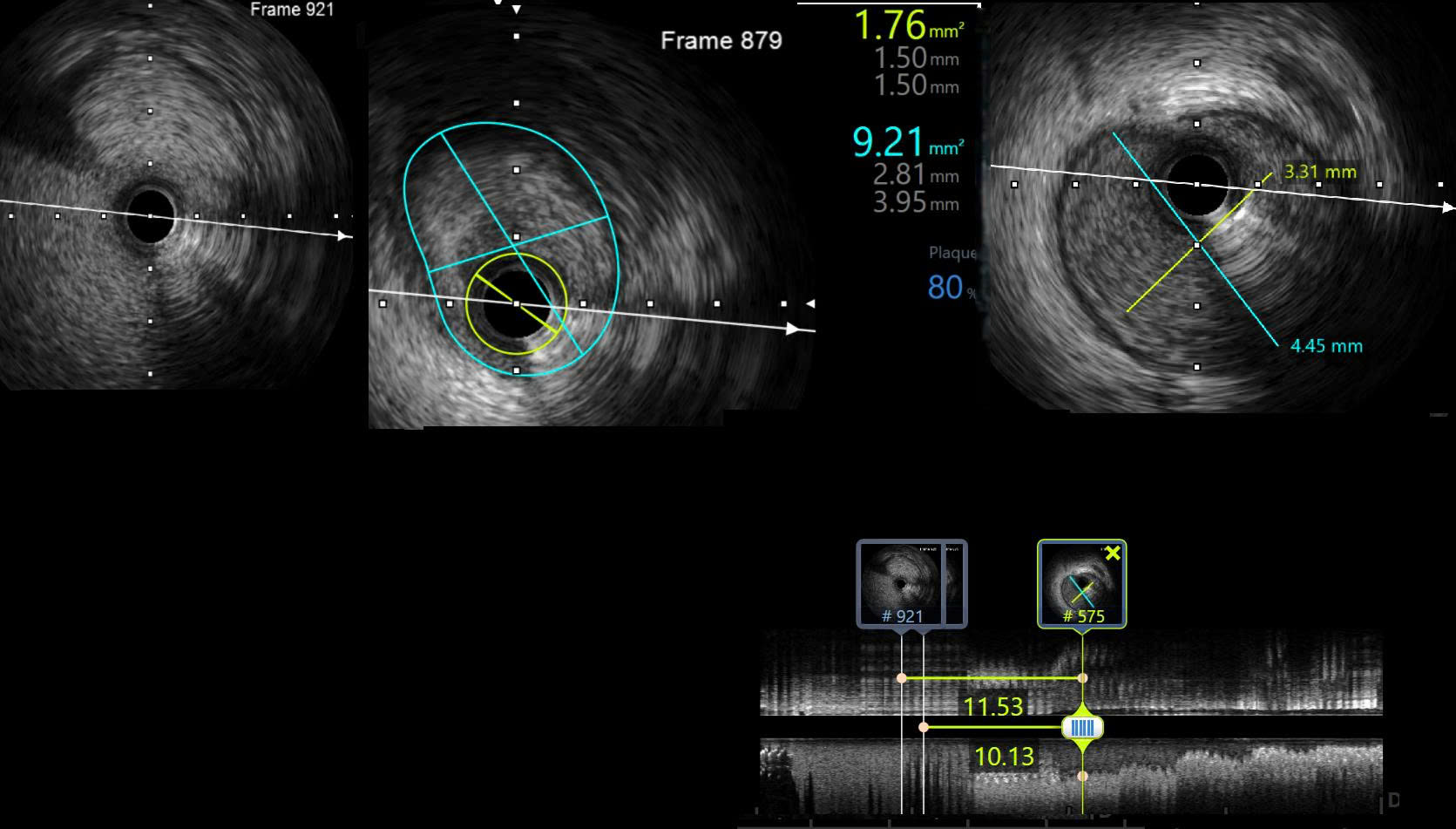
DSA and IVUS pre-intervention showed lesion located from proximal LAD to the ostium with the length of 12 mm, distal reference vessel diameter of 3.3 mm, vessel diameter of 4.4 mm. The lesion had an area of 1.76 mm2 with plaque burden of 80 %.
 20250816-1109-17.1498642.mp4
20250816-1109-17.1498642.mp4
Interventional Management
Procedural Step
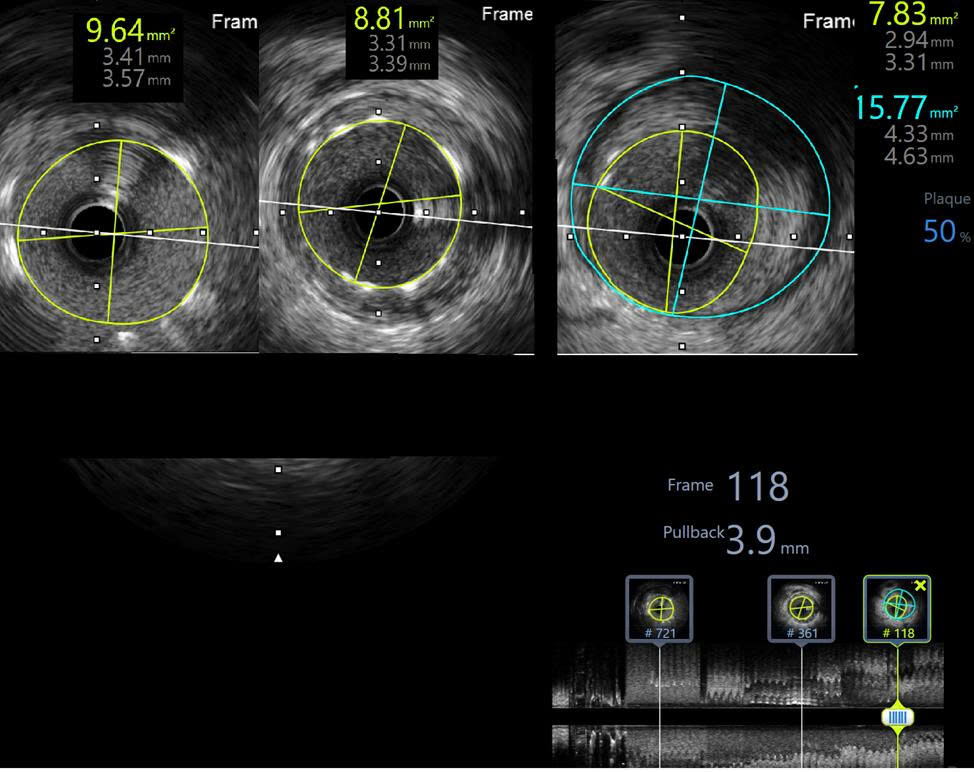
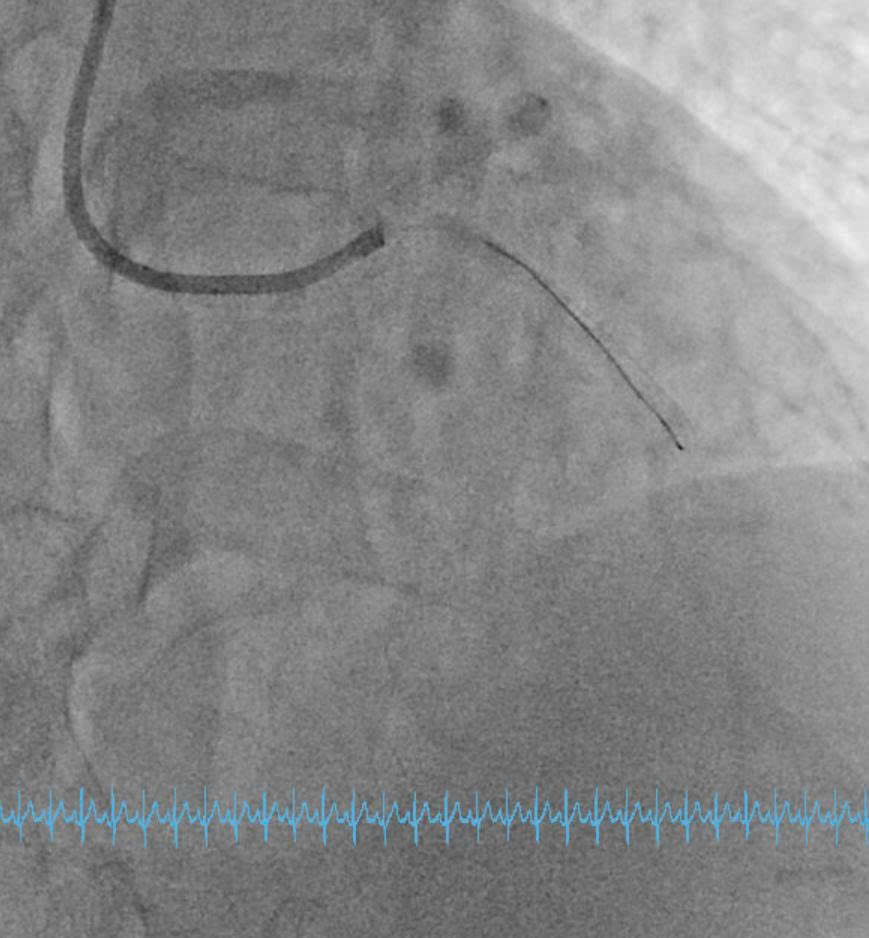
Engage the guiding catheter into the LCX ostium and advance a wire for anchoring in the LCX. After withdrawing the guiding catheter from the ostium and performing coronary angiography, it was observed that the LAD ostium originated separately from the LCX ostium and was located lower in the RAO–CRA view.Multiple attempts to selectively wire the LAD ostium using a 6 F SPB 3.0 guiding catheter (Asahi, Japan) from outside the LAD ostium were unsuccessful. The guiding catheter was then exchanged for a 6 F JL 3.5, and a Sion Blue wire was successfully advanced through the LAD ostium into the distal segment.DSA and IVUS post-intervention showed minimal stent area of 8.83 mm2, reached 112 % of distal reference vessel diameter. Stent covered LAD ostium with an area of 9.64 mm2 and was 2 mm inside the aortic artery. There was no protrusion, no dissection.
Case Summary
Absence of the left main coronary artery is a rare congenital coronary anomaly. Although generally considered benign, it can pose significant challenges during percutaneous coronary intervention, particularly in the setting of acute myocardial infarction. This anomaly may prolong procedural time and complicate the selection of appropriate catheter types and sizes. Careful assessment with intravascular imaging modalities, such as intravascular ultrasound, can facilitate accurate diagnosis and guide optimal treatment strategy. Awareness of this condition is crucial when no left main coronary artery is visualized on DSA, to ensure timely and effective revascularization.