CASE20250819_001
Conquering Ambiguous RCA Anatomy Using the Retrograde Approach and Tip-In Technique in RCA CTO PCI
By Zul Bahri, Arwin Saleh Mangkuanom, Amir Aziz Alkatiri, Nanda Iryuza, Doni Firman
Presenter
Zul Bahri
Authors
Zul Bahri1, Arwin Saleh Mangkuanom1, Amir Aziz Alkatiri1, Nanda Iryuza1, Doni Firman1
Affiliation
National Cardiovascular Centre Harapan Kita, Indonesia1
View Study Report
CASE20250819_001
Complex PCI - CTO
Conquering Ambiguous RCA Anatomy Using the Retrograde Approach and Tip-In Technique in RCA CTO PCI
Zul Bahri1, Arwin Saleh Mangkuanom1, Amir Aziz Alkatiri1, Nanda Iryuza1, Doni Firman1
National Cardiovascular Centre Harapan Kita, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 46-year-old male presented with typical chest pain that persisted despite optimal medical therapy. The patient had type 2 diabetes, hypertension, dyslipidaemia, ex-smoker status, and a history of ACS (Anterior MI) 3 months ago without revascularization. Physical examination findings were within normal limits.
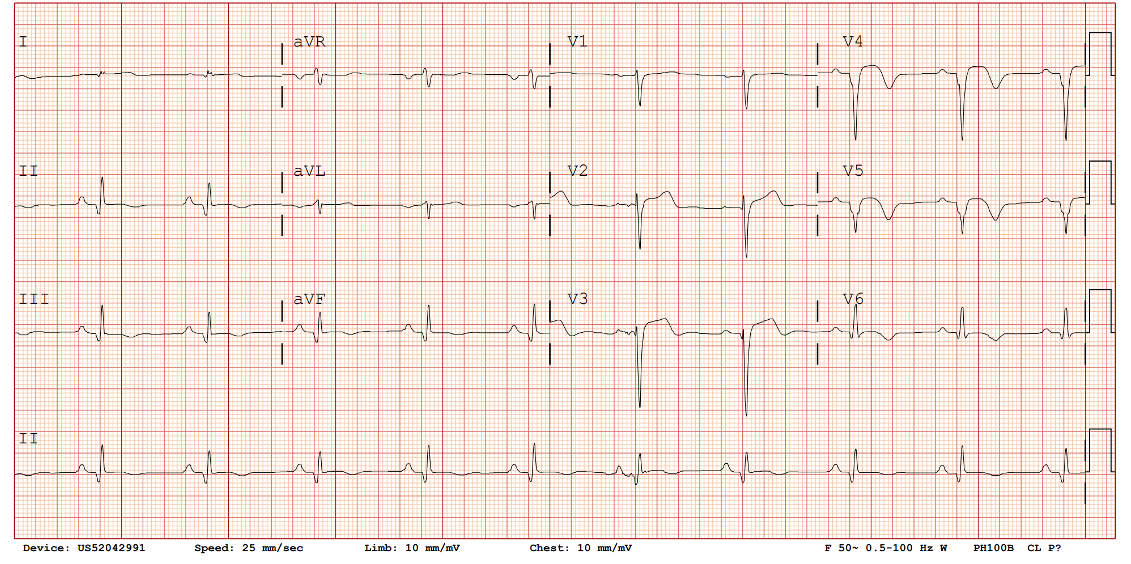
Relevant Test Results Prior to Catheterization
The ECG showed a sinus rhythm with poor R-wave progression in the anterior lead. Blood test showed Cr 1.38 (eGFR 61 ml/min). The diagnostic angiography a month before the procedure (May 2025) demonstrated chronic total occlusion at proximal RCA, moderate lesion at LAD, and small calibre non-dominant LCx.
 1 LAD 1.mov
1 LAD 1.mov
2 LAD 2.mov
3 RCA 1.mov
Relevant Catheterization Findings
The diagnostic angiography at the index PCI procedure (June 2025) demonstrated chronic total occlusion at proximal RCA with an ambiguous course, mild lesion at LAD (previously interpreted as a moderate lesion), and a small-caliber non-dominant LCx. We decided to perform PCI CTO RCA with a retrograde approach due to the ambiguity of the RCA course.
5 LCA 1.mov
6 RCA 1.mov
Interventional Management
Procedural Step
The procedure began with double arterial access via the right femoral artery (XB 3.5/7F guide catheter) and the right radial artery (JR 3.5/6F guide catheter). A workhorse wire with a microcatheter was advanced into the septal branch, followed by contrast injection, confirming a retrograde pathway to the RCA. Septal surfing was performed with a Suoh 03 wire (soft, 0.3 gr tip load), successfully reaching the distal and mid RCA. The wire exchange to an Anyreach P 1.0 wire (polymer jacketed, 1 gr tip load) and attempted to cross the distal CTO cap. Upon reaching the CTO body, the wire could not advance through the proximal cap. Escalation to an Anyreach P 6.0 wire (polymer jacketed, 6 gr tip load) successfully penetrated the proximal cap but failed to enter the guide catheter, likely due to subintimal positioning. We de-escalated to an Anyreach P 1.0 wire and successfully snared the wire into the guide catheter after several attempts. The microcatheter was advanced into the guide catheter, and the tip-in technique was successfully performed with a workhorse wire, allowing antegrade wire passage into the distal RCA. Pre-dilatation was performed using semi-compliant balloons (1.5×15 mm and 2.0×15 mm) followed by a 2.75×15 mm non-compliant scoring balloon from distal to ostial RCA. IVUS was used to assess vessel morphology and size. Three drug-eluting stents (2.75×38 mm, 3.5×20 mm, and 4.0×26 mm) were implanted from distal to ostial RCA, achieving a satisfactory final angiographic result.
Wire surfing.mov
Snaring and tip in.mov
Final Result Post Stent.mov
Case Summary
This case highlights the successful navigation of a complex proximal RCA CTO using advanced retrograde PCI techniques. Combining dual arterial access, septal surfing, wire escalation, and the tip-in technique, the team overcame anatomical challenges and an ambiguous vessel course. With IVUS guidance and careful balloon pre-dilatation, optimal stent placement was achieved, resulting in excellent revascularization. This case underscores the power of cutting-edge interventional strategies to tackle difficult CTOs and enhance patient outcomes.