CASE20250819_002
Unleashing Precision: Mastering Stent Expansion in Heavely Calcified LAD—A Journey With Rotablation and IVUS
By Katrina Ruth Ulima Hutasoit, Amir Azis Alkatiri, Nanda Iryuza, Arwin Saleh Mangkuanom, Doni Firman
Presenter
Katrina Ruth Ulima Hutasoit
Authors
Katrina Ruth Ulima Hutasoit1, Amir Azis Alkatiri1, Nanda Iryuza1, Arwin Saleh Mangkuanom1, Doni Firman1
Affiliation
National Cardiovascular Center Harapan KIta, Indonesia1
View Study Report
CASE20250819_002
Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Unleashing Precision: Mastering Stent Expansion in Heavely Calcified LAD—A Journey With Rotablation and IVUS
Katrina Ruth Ulima Hutasoit1, Amir Azis Alkatiri1, Nanda Iryuza1, Arwin Saleh Mangkuanom1, Doni Firman1
National Cardiovascular Center Harapan KIta, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
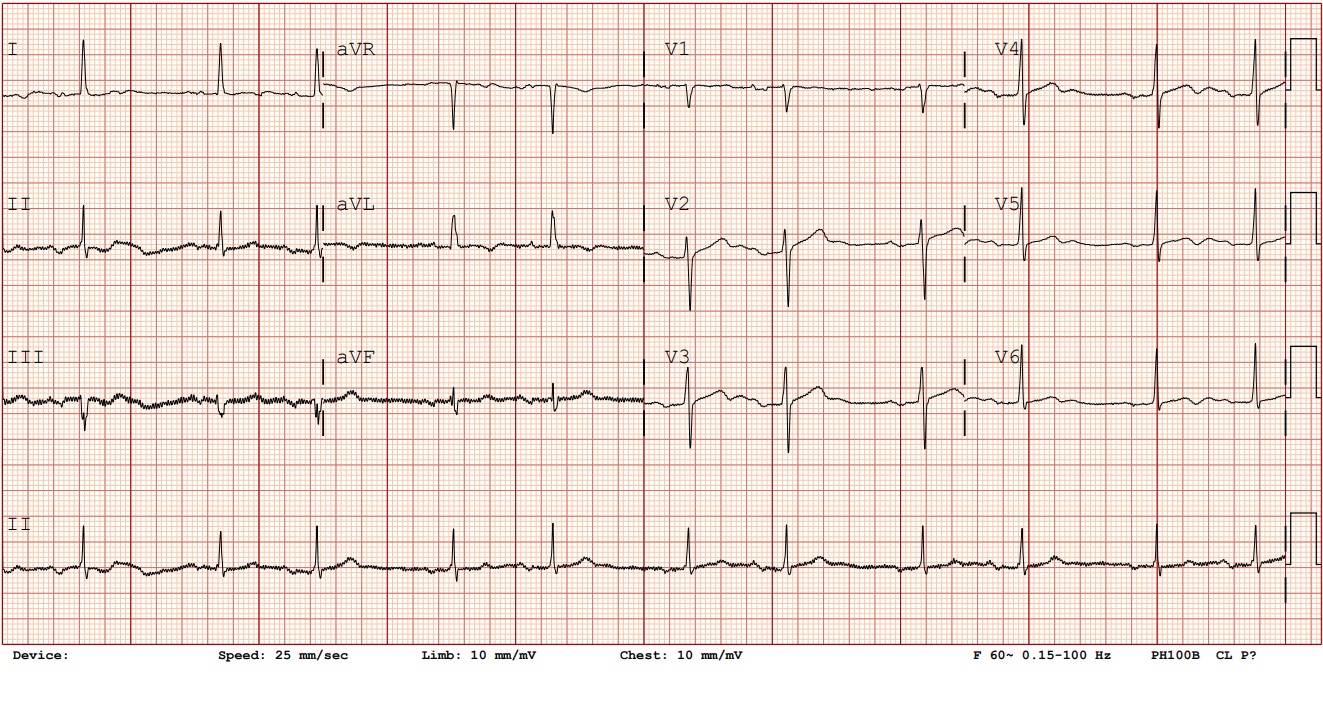
A 59 year-old male presented with angina pectoris during daily activities. The patient has a history of repeated rehospitalization 4 times within the last 5 months due to similar complaints, accompanied by a low pulse rate. Risk factors included hypertension , diabetes, obesity and dyslipidemia. Physical examination findings were within normal limits.
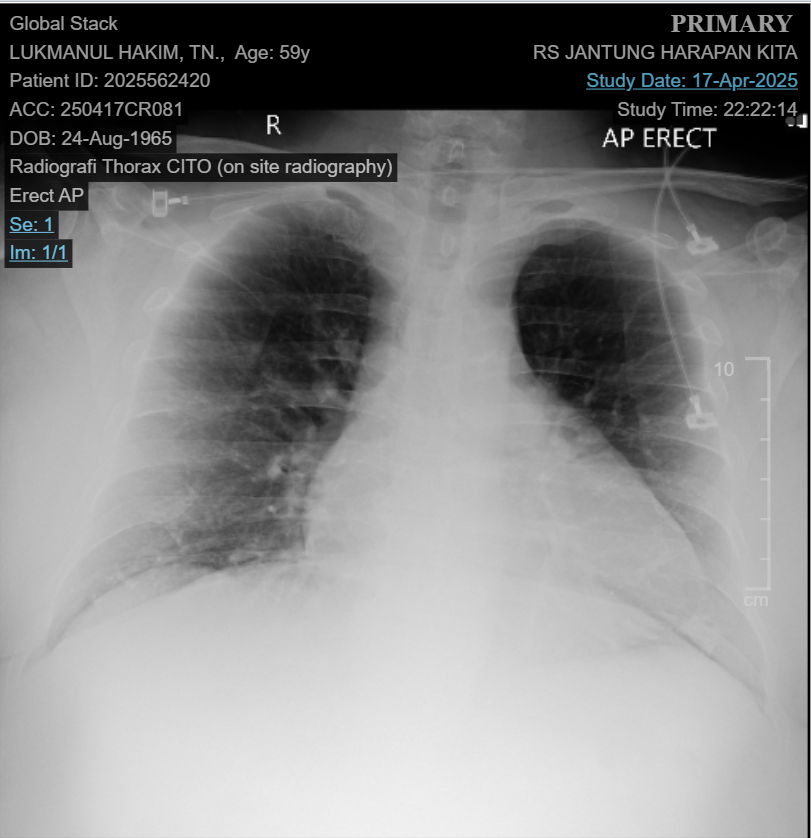
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
LM normal. LAD with calcification and diffuse stenosis from proximal–mid, with 70-80% stenosis at proximal. LCx normal with 30-50% stenosis in mid part of bifurcation OM2. RCA normal, dominant.
 RCA.mp4
RCA.mp4
LCA.mp4
Interventional Management
Procedural Step
Full-dose heparin was given. A Runthrough NS Floppy wire was advanced to the distal LAD; IVUS revealed 180-360° calcification in the proximal LAD. Using a Finecross microcatheter, the wire was exchanged for a Rota Floppy wire. Rotational atherectomy was performed with a 1.75 mm burr at 180,000 rpm, followed by polishing at 140,000 rpm in the proximal to mid LAD. IVUS showed calcium cracks with reverberation. Predilatation with a 2.5×15 mm cutting balloon at 16 atm caused balloon burst in the proximal LAD. Double wiring was done with Runthrough NS Floppy wires in the distal LAD and diagonal artery. Predilatation with a 3.0×15 mm scoring balloon at 20 atm . Predilatation was repeated with 2.75×15 mm cutting balloon also caused balloon burst in the proximal LAD. Predilatation with 3.0×15 mm scoring balloons at 20 atm with good results. IVUS showed multiple calcium fractures and an adequate lumen. A DES 3.0×28 mm stent was implanted using a 5.5 F guide extension and inchworm technique due to insertion difficulty. The stent was delivered successfully to mid LAD, overlapped proximally with a DES 3.5×28 mm. Post-dilation with a 3.5×15 mm NC balloon was done at high pressure. Angiography showed good results; IVUS confirmed no dissection, well apposed and expanded stent with MSA of 9.15 mm². Procedure completed without complications. Total contrast 240 ml, fluoroscopy time 27 min, dose area product 119 Gy·cm².
ROTA.mp4
Balloon.mp4
Stent dan angiography.mp4
Case Summary
A patient with severely long calcified LAD lesion. Using rotational atherectomy, cutting and scoring balloon angioplasty, and IVUS-guided DES implantation, we achieved successful complete revascularization. With regard to atheroablative strategies, RA can effectively modify calcified plaque and smooth the vessel lumen to enable subsequent balloon dilatation and stent implantation. When combined with IVUS guidance, it allows precise lesion assessment and ensures optimal stent deployment, ultimately improving patient prognosis.