CASE20250819_003
A Challenging Case of Calcified Lesion in Right Coronary Artery
By Chun-Chieh Liu, Li Yen, Liang Hsu Liu, Chun-Wei Lee
Presenter
Li Yen
Authors
Chun-Chieh Liu1, Li Yen1, Liang Hsu Liu1, Chun-Wei Lee1
Affiliation
Mackay Memorial Hospital, Taiwan1
View Study Report
CASE20250819_003
Complex PCI - Calcified Lesion
A Challenging Case of Calcified Lesion in Right Coronary Artery
Chun-Chieh Liu1, Li Yen1, Liang Hsu Liu1, Chun-Wei Lee1
Mackay Memorial Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
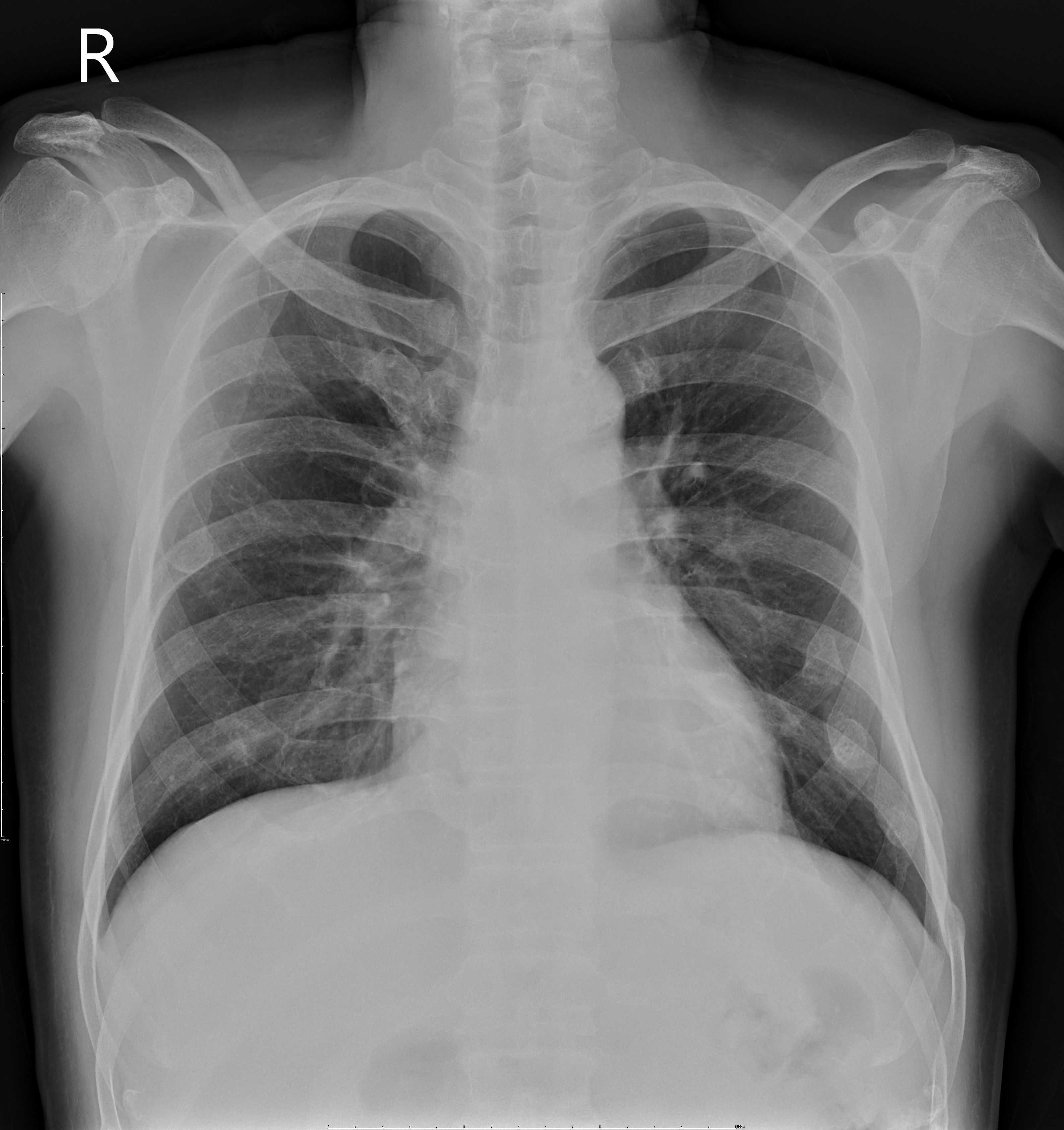
A 63-year-old male with a medical history of poorly controlled type 2 diabetes, hypertension, stage III chronic kidney disease, and a previous non-ST elevation myocardial infarction (NSTEMI) treated with drug-eluting stents, presented to the emergency department with recurrent chest tightness, which lasted approximately 10 minutes. Upon examination, his vital signs were stable, and his heart rhythm was regular with normal heart sounds and no murmurs. Lung auscultation was clear bilaterally.
Relevant Test Results Prior to Catheterization
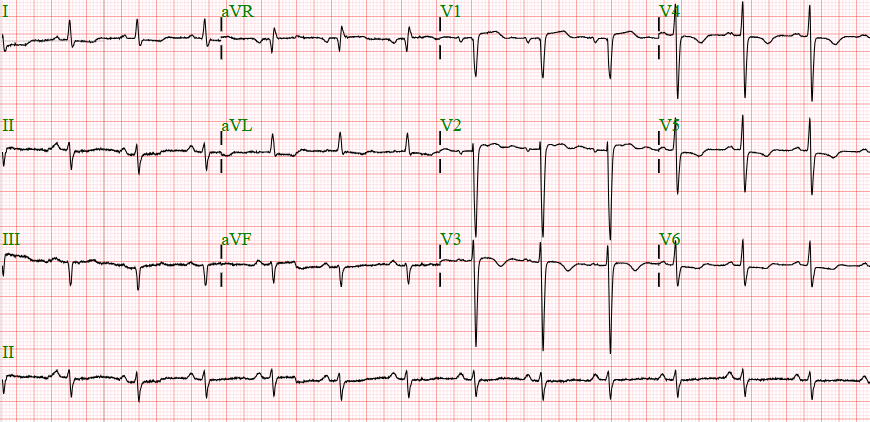
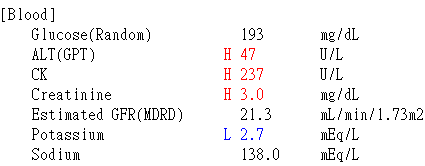
EKG revealed normal sinus rhythm with myocardial ischemic change. Laboratory data demonstrated elevated cardiac enzyme and impaired renal function. Initial transthoracic echocardiography revealed anterior wall motion abnormality with impaired left ventricle systolic function.

 heart sonography.mp4
heart sonography.mp4
Relevant Catheterization Findings
Coronary angiography revealed 99% in-stent restenosis in the proximal left anterior descending artery (p-LAD) and 90% stenosis in the mid right coronary artery (RCA). Intervention for the RCA lesion was challenging, as the balloon could not cross the stenotic segment despite multiple attempts or techniques. Severe calcification was suspected to be the major obstacle.
balloon.mp4
balloon 2.mp4
balloon 3.mp4
Interventional Management
Procedural Step
Given the balloon-uncrossable lesion, rotational atherectomy was considered necessary to facilitate stent delivery and proper expansion. However, the heavily calcified plaque was located at a curvature of the RCA, raising the risk of complications with multiple burr passes. In addition, the patient’s cardiac and renal function was compromised, and even minor complications could have resulted in life-threatening consequences. Therefore, a combined strategy of rotational atherectomy and intravascular lithotripsy (IVL) was planned after thorough discussion.A temporary pacemaker was placed first as backup before initiating the procedure. The microcatheter could not cross the lesion, thus a direct wiring technique with a RotaWire was performed. Rotational atherectomy was carried out with a 1.25 mm burr at high speed (176,000–178,000 rpm). Episodes of bradycardia occurred but the lesion was successfully crossed. Intravascular ultrasound (IVUS) revealed severe calcification with 270° arc in the distal LAD and 360° in the mid LAD, with partial fracture. IVL was delivered to the distal RCA, followed by liquefaction of the calcium from d-RCA to m-RCA. Non-compliant balloon predilatation was then performed, and repeat IVUS confirmed multiple cracks with significant luminal gain. Two drug-eluting stents were deployed according to measurement from IVUS. After adequate post-dilatation, IVUS confirmed optimal stent expansion with good apposition and no edge dissection.
rotablation.mp4
IVL.mp4

Case Summary
This complex, heavily calcified lesion located in right coronary artery was treated efficiently without major complications and the patient tolerated the procedure well. Total contrast amount was eighty milliliter, and the procedure time was two and half hours. Our case confirmed a combined strategy of rotational atherectomy and intravascular lithotripsy was both safe and feasible, especially in compromised heart and high risk patient.