CASE20250820_002
Spasm, Occlusion, Dissection, Percutaneous Transluminal Coronary Angioplasty of the Right Coronary Artery
By Konstantin Zavialov, Marat Karimov, Sergei Blagodarov, Levon Arzumanyan
Presenter
Konstantin Zavialov
Authors
Konstantin Zavialov1, Marat Karimov1, Sergei Blagodarov1, Levon Arzumanyan1
Affiliation
Bashkir State Medical University Clinic, Russian Federation1
View Study Report
CASE20250820_002
Complication Management - Complication Management
Spasm, Occlusion, Dissection, Percutaneous Transluminal Coronary Angioplasty of the Right Coronary Artery
Konstantin Zavialov1, Marat Karimov1, Sergei Blagodarov1, Levon Arzumanyan1
Bashkir State Medical University Clinic, Russian Federation1
Clinical Information
Relevant Clinical History and Physical Exam
Patient T, 71 years old. Has suffered from hypertension for a long time. His condition has been deteriorating for the last 6 months. Complaints: pressing pain behind the breastbone, radiating to the neck, occurring when walking less than 200 meters and during emotional stress, relieving on its own at rest, accompanied by shortness of breath, attacks of rapid heartbeat, shortness of breath when walking around the house, general weakness
Relevant Test Results Prior to Catheterization
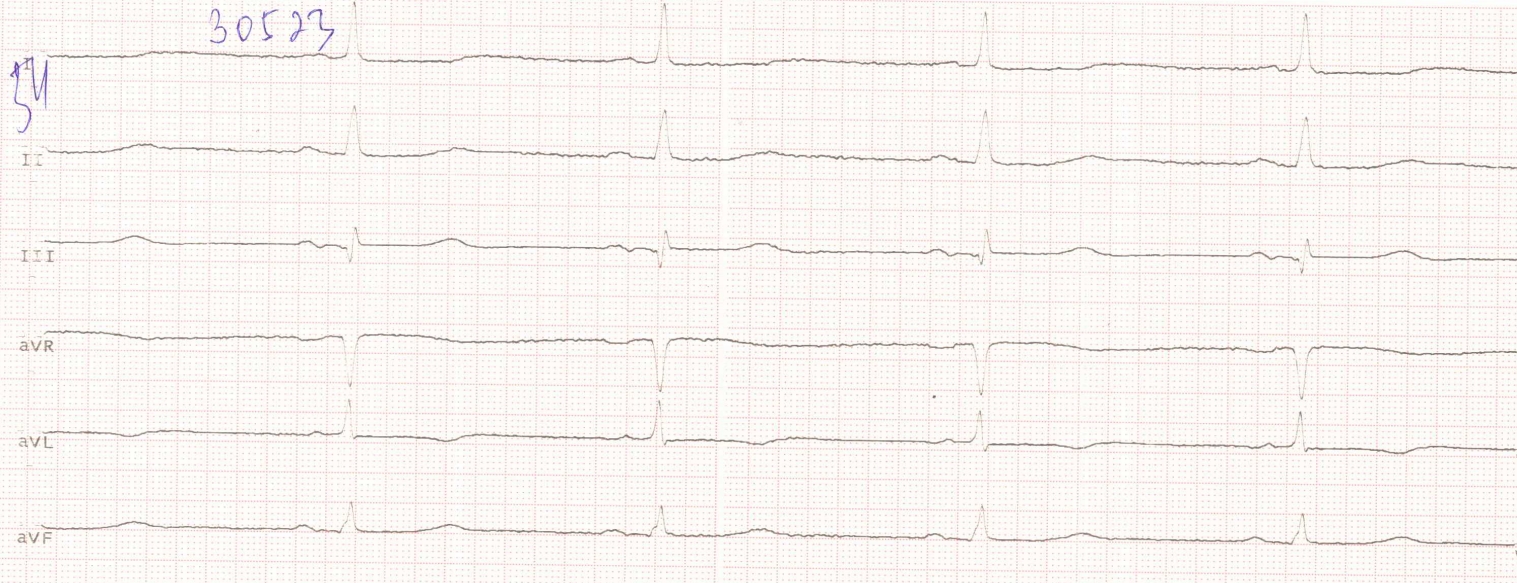
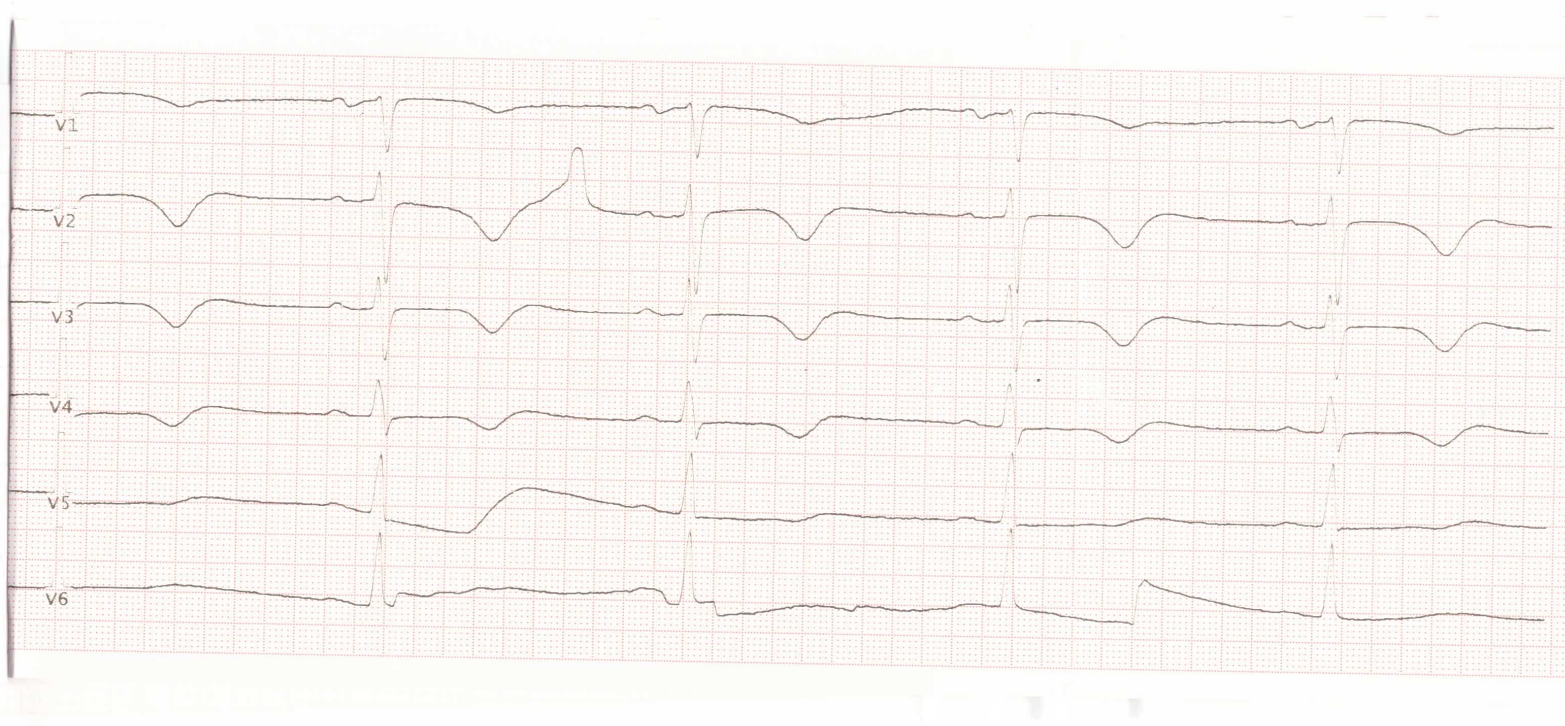
Sinus rhythm, heart rate 54 beats/min. Bradycardia. EOS is not deviated. Violation of repolarization processes due to ischemia in the myocardium of the anterior-septal-apical region of the left ventricle.
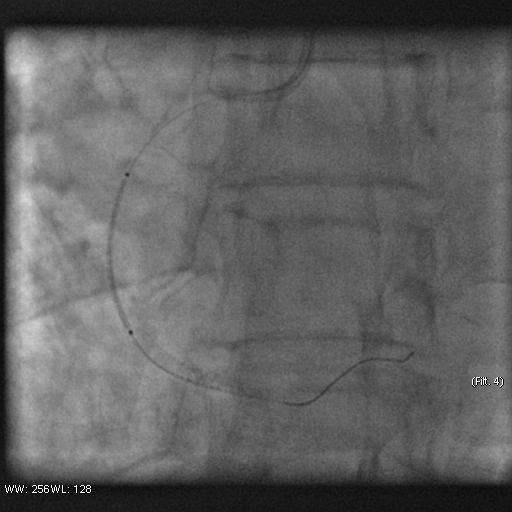
Relevant Catheterization Findings
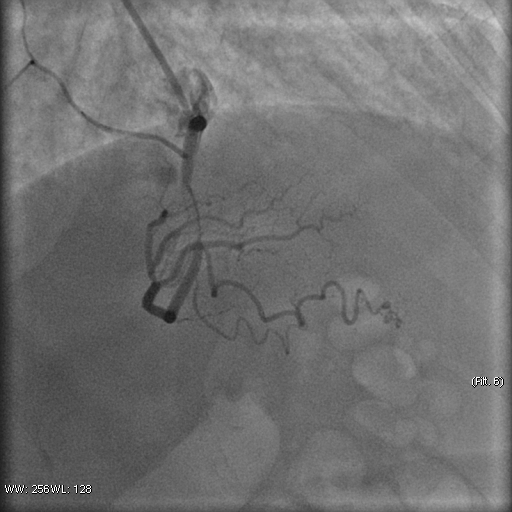
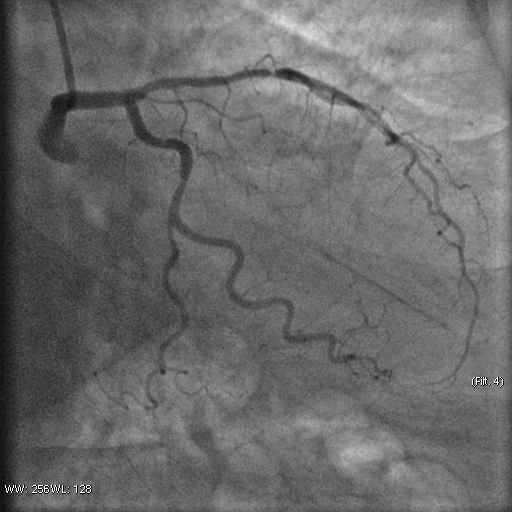
Stenosis of the anterior interventricular artery in the 6.7 segment is 95%. Stenosis of the orifice of the diagonal artery of the 1st order is 95%. Stenosis of the circumflex artery in the 13th segment is 40%. During coronary angiography, pronounced spasm is noted in the 2nd segment of the right coronary artery with complete occlusion of the artery lumen. After stopping the spasm, coronary angiography shows a spiral (spontaneous) dissection of the right coronary artery from segments 1 to 3.

Interventional Management
Procedural Step
A guiding catheter JR 3.5 6Fr was inserted along a 0.035" 260.0 cm guidewire. The guidewire was removed. The right coronary artery was catheterized. A 7Fr Y-click connector (complete with an insertion device and a guidewire rotation device) was connected to the guiding catheter. A coronary guidewire Whisper ES 0.014" 190 cm, Asahi Gaia Third 0.014" 190 cm was inserted and brought into the orifice of the right coronary artery. The guidewire was inserted beyond the lesion zone of the right coronary artery in segment 2, then into the distal sections. Wilma NC 2.00*20.0 mm and Wilma NC 3.00*15.0 mm balloon catheters were inserted alternately along the coronary guidewire - predilation of the lesion zone of the right coronary artery in segment 2 was performed. Inflation of balloon catheters 14 atm. with an inflator, the balloon catheters are deflated and removed. A stent is inserted along the coronary guidewire - the Yukon Chrom PC 3.0 * 28.0 mm system, Yukon Chrom PC 3.0 * 28.0 mm, Cid Cre 8 3.50 * 25.0 mm, Cid Cre 8 4.0 * 16.0 mm - the stent is implanted in the lesion area of the right coronary artery in the 2nd segment. Inflation of the balloon catheter 9-16 atm. with an inflator, the balloon catheter is deflated and removed. Control coronary angiography - blood flow in the stenting zone is TIMI3, there are no signs of dissection or stent dislocation.


Case Summary
1. Do not overestimate your capabilities and skills during percutaneous coronary intervention2. Never work in the coronary arteries without having the entire range of stents3. It is important to assess the condition of the coronary arteries in all projections