CASE20250820_006
Revascularization of LAD Dissection in a Patient With Recurrent ST-Elevation Myocardial Infarction After Surviving Cardiac Arrest in Staged PCI
By HANG LONG LI, Pak Hin Tam, TSUN HO LAM, WANG HEI RICKY LEUNG, CHEUNG CHI SIMON LAM, CHOR CHEUNG FRANKIE TAM
Presenter
Pak Hin Tam
Authors
HANG LONG LI1, Pak Hin Tam1, TSUN HO LAM1, WANG HEI RICKY LEUNG2, CHEUNG CHI SIMON LAM1, CHOR CHEUNG FRANKIE TAM1
Affiliation
Queen Mary Hospital, Hong Kong, China1, Queen Mary Hospital, Honduras2
View Study Report
CASE20250820_006
ACS/AMI - ACS/AMI
Revascularization of LAD Dissection in a Patient With Recurrent ST-Elevation Myocardial Infarction After Surviving Cardiac Arrest in Staged PCI
HANG LONG LI1, Pak Hin Tam1, TSUN HO LAM1, WANG HEI RICKY LEUNG2, CHEUNG CHI SIMON LAM1, CHOR CHEUNG FRANKIE TAM1
Queen Mary Hospital, Hong Kong, China1, Queen Mary Hospital, Honduras2
Clinical Information
Relevant Clinical History and Physical Exam
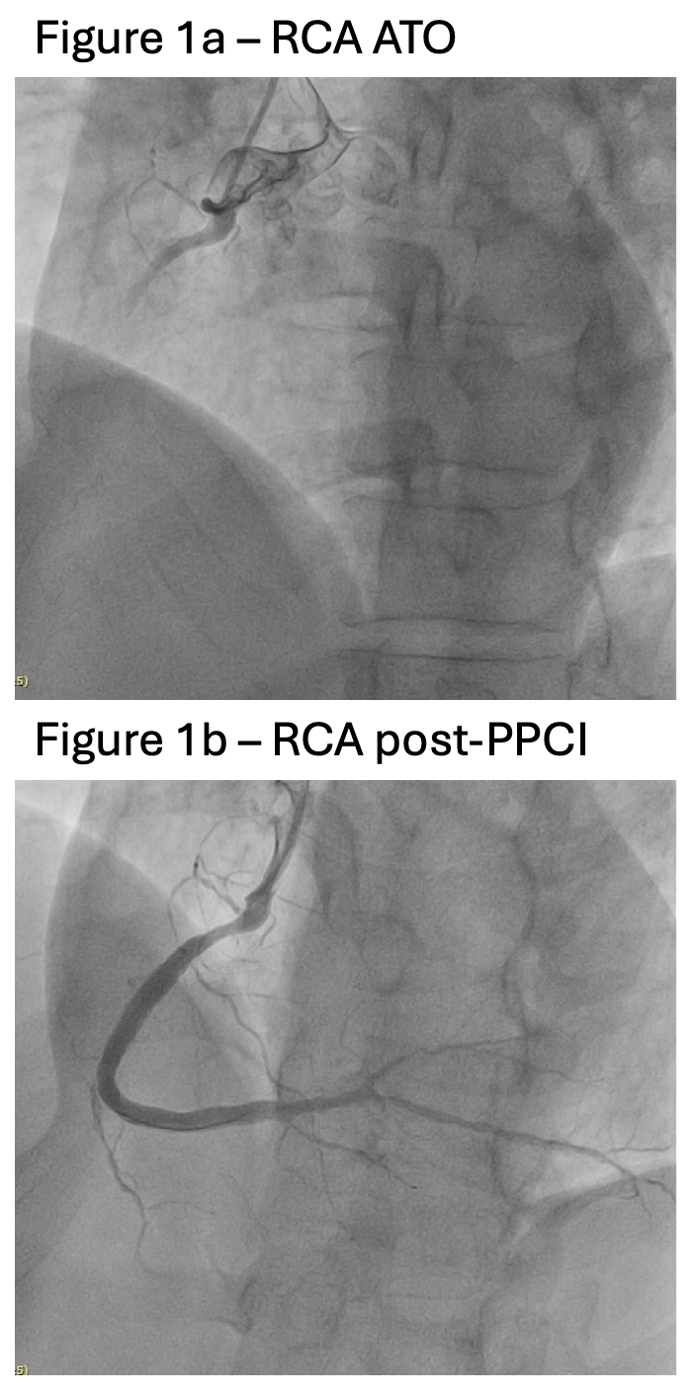
A 56-year-old male diabetic underwent primary PCI to RCA (Figure 1). In staged PCI, after revascularization to LCX, there was spontaneous plaque rupture over LAD complicated with no flow and cardiac arrest, and it was managed with plain old balloon angioplasty with Impella CP support (Video 1). OCT revealed lipid-rich plaque (Video 2). After stabilization, the patient refused further invasive intervention. One month later, he presented with acute onset of chest pain with cardiogenic shock.
 Video 1.mov
Video 1.mov
Video 2.mov
Relevant Test Results Prior to Catheterization
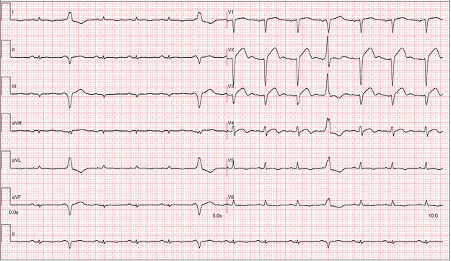
ECG of the patient showed ST elevation over anterior leads (Figure 2). Echocardiogram revealed left ventricular ejection fraction (LVEF) of 20% with global hypokinesia worse over apical region. Point-of-care testing revealed elevated serum troponin level.The low-density lipoprotein level remained elevated despite intensive lipid-lowering therapy with statin and Evolocumab, the latter of which was initiated after staged PCI. These might have contributed to the lipid-rich nature of the plaque.
Relevant Catheterization Findings
Cardiac catheterization revealed dissection flap over proximal LAD, with diffuse severe stenosis along proximal, mid, and distal LAD. There was mild stenosis over LM. There was moderate stenosis over ostial and distal LCX, with severe focal stenosis over distal OM. There was focal moderate stenosis over distal RCA and with diffuse stenosis over PDA/PL. There was no significant in-stent restenosis over RCA/LCX.
Interventional Management
Procedural Step
The LM was engaged with 6Fr EBU3.5 guiding catheter via RFA. Boluses of Eptifibatide were given. Aspiration thrombectomy was performed with Eliminate, yielding a considerable amount of thrombi. The LAD lesion was pre-dilated with SC 2.0 balloon. The patient then developed further decompensated cardiogenic shock requiring high dose inotropes, and intra-aortic balloon pump (IABP) was inserted (Video 3).Intravascular ultrasound (IVUS) of the LAD confirmed showed evidence of plaque rupture over proximal LAD (Video 4). The lesion was further pre-dilated with NC 3.0 balloon, followed by stenting by Ultimaster nagomi 3.5/28 and 3.0/24. Post-dilatation was performed with NC 3.0, NC 3.5, and NC 3.75 balloons sequentially. Angiogram and IVUS revealed excellent results (Video 5).
Video 3.mov
Video 4.mov
Video 5.mov
Case Summary
During staged PCI, the patient had spontaneous LAD plaque rupture resulting in no flow and cardiac arrest requiring mechanical circulatory support. He was managed with intracoronary adrenaline and nitroprusside but refused further intervention after stabilization. He subsequently developed anterior STEMI with cardiogenic shock requiring IABP as a result of proximal LAD dissection and plaque rupture, and was successfully treated aspiration thrombectomy in addition to Eptifibatide followed by stenting. One month after revascularization, the LVEF improved to 35%.This case highlights the potential risk conferred by lipid-rich plaque, and the importance of definitive intervention.