CASE20250820_010
Non-Culprit Lesion Intervention in Acute Myocardial Infarction With Cardiogenic Shock in the Absence of Mechanical Support
By Chinh Duc Nguyen, Thi Phuong Anh Nguyen, Cong Dinh Pham, Thi Quynh Huong Tran
Presenter
Thi Phuong Anh Nguyen
Authors
Chinh Duc Nguyen1, Thi Phuong Anh Nguyen1, Cong Dinh Pham1, Thi Quynh Huong Tran1
Affiliation
Stroke International Services General Hospital, Vietnam1
View Study Report
CASE20250820_010
High-Risk Intervention - High-Risk Intervention (Diagetes, Heart Failure, Renal Failure, Shock, etc)
Non-Culprit Lesion Intervention in Acute Myocardial Infarction With Cardiogenic Shock in the Absence of Mechanical Support
Chinh Duc Nguyen1, Thi Phuong Anh Nguyen1, Cong Dinh Pham1, Thi Quynh Huong Tran1
Stroke International Services General Hospital, Vietnam1
Clinical Information
Relevant Clinical History and Physical Exam
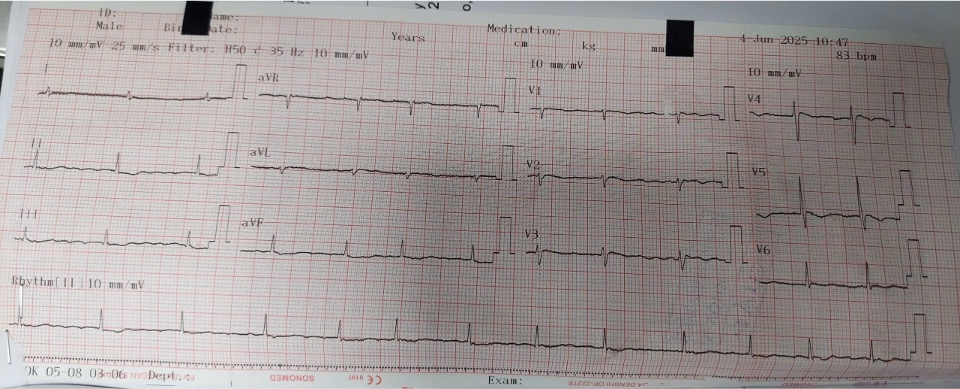
A 87-year-old man was admitted for shortness of breath. The patient had productive cough with green sputum and no fever two days before admission. He was diagnosed with moderate pneumonia at the outpatient clinic and given oral antibiotics. Progressive dyspnea without fever led to hospitalization on admission.
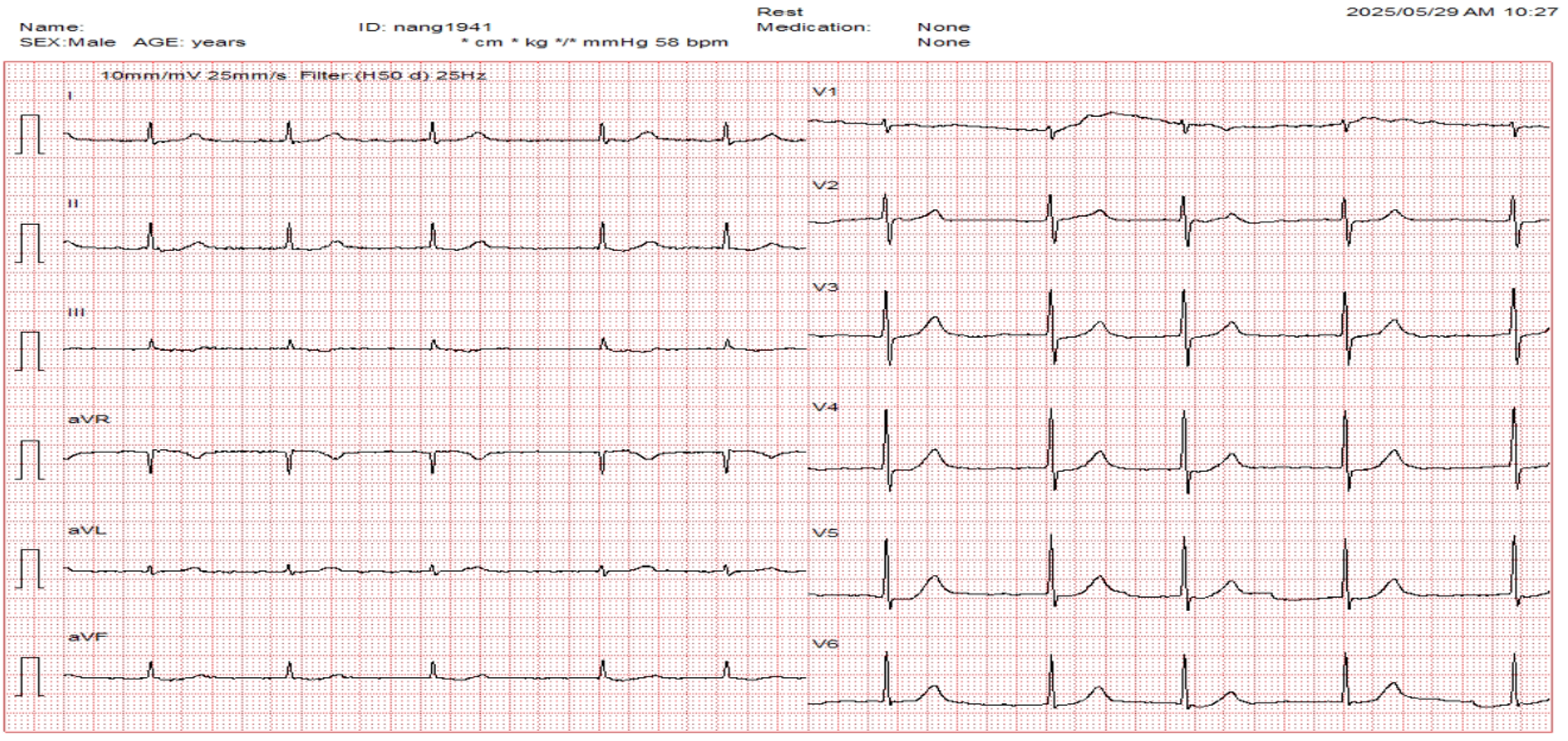
Relevant Test Results Prior to Catheterization
MRI brain imagings were limited by poor cooperation, however DWI revealed a fresh right cerebral hemisphere infarct. Right hemisphere cerebral infarction and pneumonia were listed.
Relevant Catheterization Findings
A 6F Radifocus introducer sheath was inserted via the right radial artery. Using an Osprey 5F catheter x02 and Advance system, we found: Right dominant coronary system. LMCA: 40% stenosis. LAD: 90% stenosis in segment I, 90% stenosis in segment II. LCx: 80% stenosis in segment I. RCA: 50% stenosis in segment I,subtotal occlusion in RCA II, collaterals from Septal and LCX with Rentrop 2; 90% stenosis in segment III, 70% stenosis in PLV, 80% stenosis in PDA.
 DSA 3.mp4
DSA 3.mp4
DSA 2.mp4
DSA 1.mp4
Interventional Management
Procedural Step
RCA II–III via right radial artery with 7F catheter.
PCI 3.mp4
PCI 2.mp4
PCI 1.mp4
Case Summary
Management of non-culprit lesions in the setting of acute myocardial infarction complicated by cardiogenic shock remains controversial. Current evidence generally supports a culprit-only approach in the acute phase, as multivessel intervention may increase procedural time, contrast load, and hemodynamic instability, particularly in the absence of mechanical circulatory support. However, in selected cases with critical non-culprit stenoses, staged or carefully performed intervention may be necessary to optimize clinical outcomes. Our case highlights the importance of individualized decision-making, balancing immediate hemodynamic risk against long-term myocardial salvage.