CASE20250821_004
Unusual Complication of Rotational Arthrectomy: Helical-Shaped Flesh Fragment During Percutaneous Coronary Intervention
By Surenthiran Ramanathan, Navindran Selvaraju, Asri Ranga Abdullah Ramaiah
Presenter
Surenthiran Ramanathan
Authors
Surenthiran Ramanathan1, Navindran Selvaraju1, Asri Ranga Abdullah Ramaiah1
Affiliation
Hospital Sultan Idris Shah Serdang, Malaysia1
View Study Report
CASE20250821_004
Complex PCI - Calcified Lesion
Unusual Complication of Rotational Arthrectomy: Helical-Shaped Flesh Fragment During Percutaneous Coronary Intervention
Surenthiran Ramanathan1, Navindran Selvaraju1, Asri Ranga Abdullah Ramaiah1
Hospital Sultan Idris Shah Serdang, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 63-year-old Malaysian Malay male, with type 2 diabetes mellitus and hypertension, stable on medications, was referred for coronary assessment following detection of a high calcium score on CT-screening (1159). Clinical findings were unremarkable. He has angina on exertion, CCS I - II.

Relevant Test Results Prior to Catheterization
LV Ejection Fraction 61.9% and normal otherwise. Haemoglobin 14.6 g/dL, Platelet 366 X10^3/uL , Creatinine 65 umol/L with eGFR >90ml/min, LDL 1.84 mmol/L.Blood pressure was 134/77 mmHg and pulse rate was 68 blm.Chest xray was normal , electrocardiogram was normal sinus rhythm.
Relevant Catheterization Findings
Catheterisation findings showed LAD: 70% proximal to mid stenosis with calcificationLCx: 80% distal stenosis and RCA (dominant) : 80% proximal to mid long, diffuse stenosis.
He was first planned for a Staged PCI to the LAD.If successful then staged PCI to RCA much later.
 Diagnostic of LAD-mov-series-009-Coronary 15fps Medium.wmv
Diagnostic of LAD-mov-series-009-Coronary 15fps Medium.wmv
Diagnostic of LCx-mov-series-010-Coronary 15fps Medium.wmv
Diagnostic of RCA-mov-series-006-Coronary 15fps Medium.wmv
He was first planned for a Staged PCI to the LAD.If successful then staged PCI to RCA much later.
Interventional Management
Procedural Step
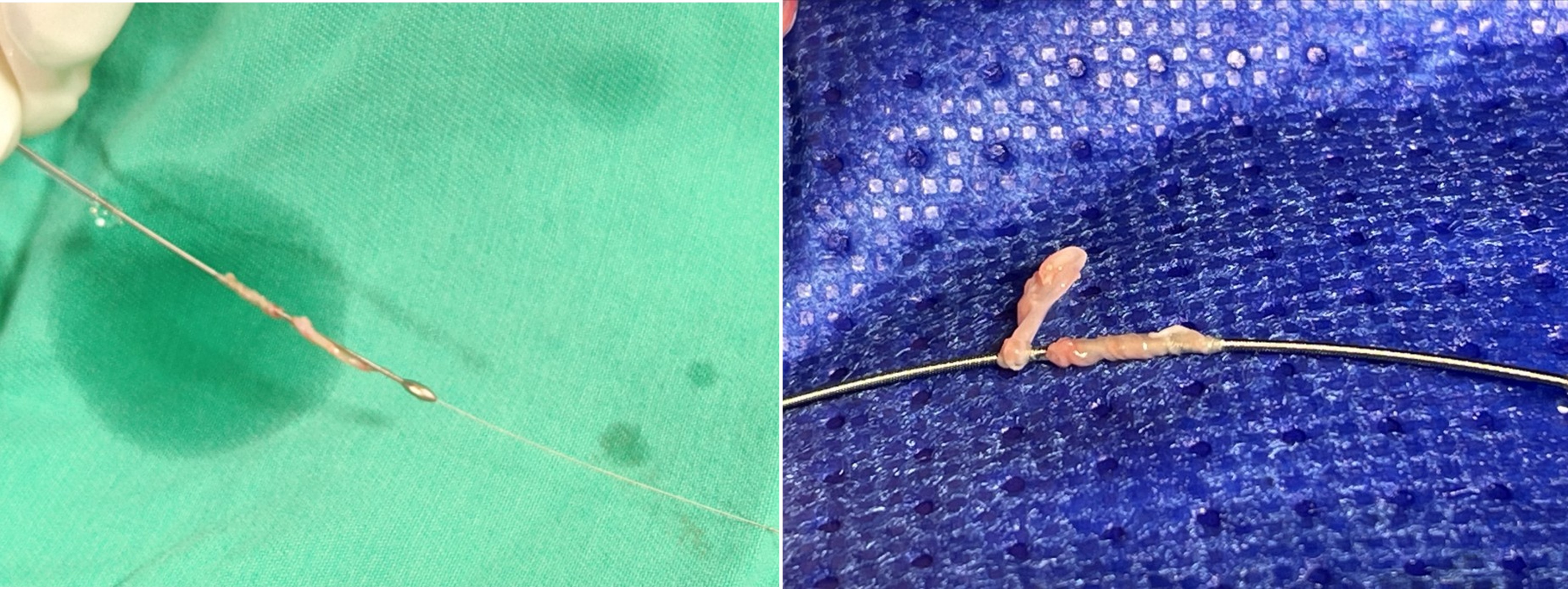
Using a 6Fr EBU 3.0 guiding catheter and Asahi Sion Blueguidewire, the operator encountered significant resistance crossing the heavilycalcified lesion. Predilatation with semi-compliant balloons (2.0/15mm) was difficulteven with guide extension and had limited success. IVUS could only be passeddown half way and showed an lumen area of 8.16 mm² much proximal to thetightest lesion. Due to the lesion’s complexity, rotational atherectomy wasperformed with a Boston Scientific ROTAPRO 1.5Burr at 180,000 rpm. During thefirst pass, resistance was encountered mid-LAD, causing the burr to becomelodged. Excessive retrieval force led to transient ventricular asystole, whichwas promptly managed with brief CPR ( less than 1 minute ) and guidewires dislodging. Subsequent cineangiographyrevealed significant dissection midLAD. The entire burr system was removed and inspectionof the burr tip revealed a remarkable, approximately 7 cm long, helical-shapedtissue fragment— suggestive of tissue shearing. Furtherpredilatation was completed with a scoring balloon (3.0/15mm). Full stentdeployment (3.0/38mm drug-eluting stent) from proximal to mid-LAD was achieved,followed by sequential post-dilatation with larger non-compliant balloons (3.5/15mm,4.0/15mm, 4.5/6mm). Final IVUS confirmed optimal stent expansion andapposition, with tightest area minimal cross-sectional areas of 6.51 mm² and7.21 mm². The patient recovered uneventfully and was discharged 48hours later.
Rota bit stuck-mov-series-020-Fluoroscopy.wmv
final shots-mov-series-053-Coronary 15fps Medium.wmv
Case Summary
The visualization of a large, helix-shaped tissue fragmentattached to the burr suggests that resistance during device maneuvering caninduce vessel wall or lesion tissue shearing. Such fragments pose a significantrisk for distal embolization and downstream ischemia. The literature, includingWilliams et al. (2014), Krasuski et al. (2013), and Kumar et al. (2018),supports that while rotational atherectomy is generally safe, operatorvigilance is essential. This case highlights the importance of cautious devicehandling during rotational atherectomy, particularly when resistance isencountered to avoid fatal complications.