CASE20250821_006
IVUS Guided Long Segment Ostial Left Anterior Descending Chronic Total Occlusion With Ambiguous Stump and Left Main Bifurcation Stenting
By Ankur Gupta
Presenter
Ankur Gupta
Authors
Ankur Gupta1
Affiliation
PGIMER, India1
View Study Report
CASE20250821_006
Complex PCI - CTO
IVUS Guided Long Segment Ostial Left Anterior Descending Chronic Total Occlusion With Ambiguous Stump and Left Main Bifurcation Stenting
Ankur Gupta1
PGIMER, India1
Clinical Information
Relevant Clinical History and Physical Exam
This 50 years old hypertensive male patient with previous Acute Coronary Syndrome 3 years back, presented with worsening angina on exertion NYHA class III for last 3 months.

Relevant Test Results Prior to Catheterization
Echocardiography revealed LAD territory hypokinesia and LVEF of 45 %.
Relevant Catheterization Findings
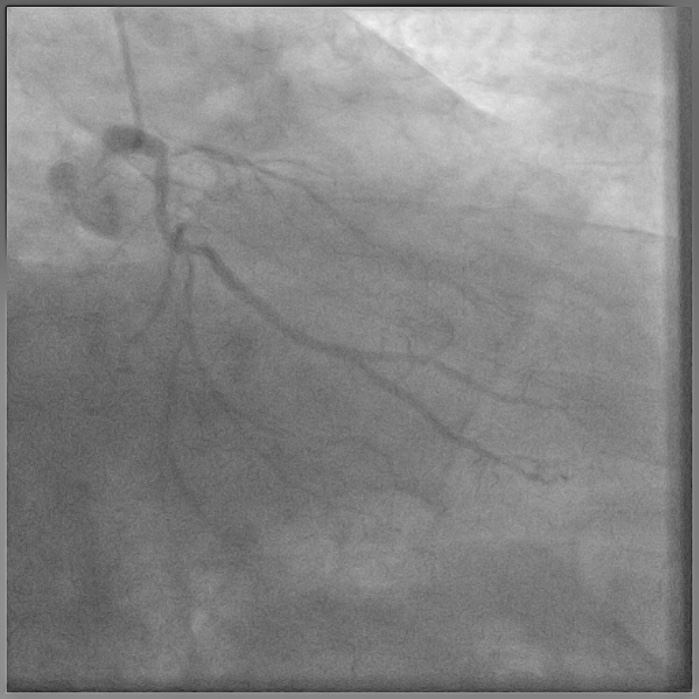
Coronary angiography done outside showed normal LM, ostial LAD cut off with retrograde filling from RCA via Grade 2 collaterals, ostial Lcx 90% stenosis (D1,D2) , large normal OM1, small and diffusely diseased OM2 and OM3, dominant RCA showing mid plaque and distal 50 % stenosis (D3).


Interventional Management
Procedural Step
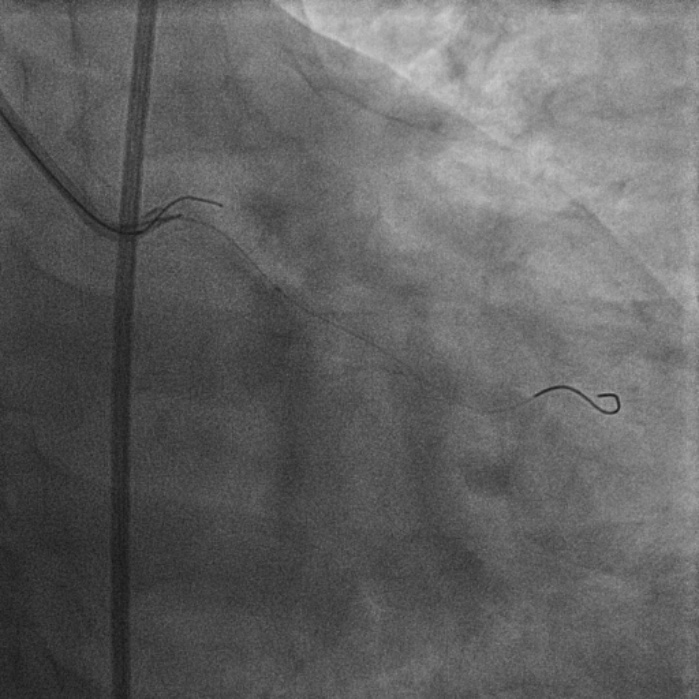
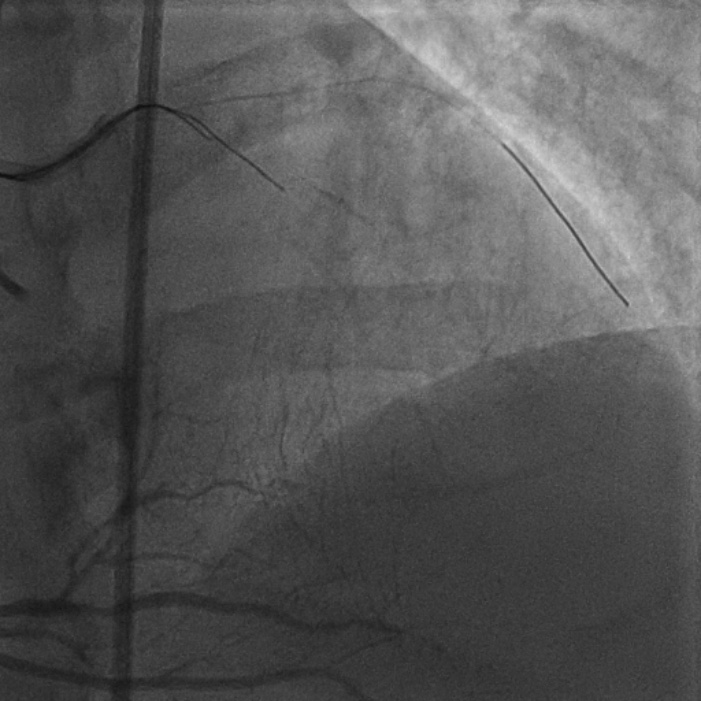
8F JL coronary guide catheter was taken from the right femoral artery and a TIG diagnostic catheter was taken from right radial artery and bilateral angiograms were taken. A floppy guide wire was placed in Lcx and ostial Lcx lesion was predicated with a 2*12 mm non compliant balloon. An IVUS catheter was placed over Lcx wire and under IVUS guidance a Gaia 3 coronary wire (Asahi, Japan) over a micro catheter was used to probe the ambiguous osmium of LAD (T1). Using contralateral injection in RCA, the Gaia 3 wire was seen extending into the false lumen in distal LAD. A Conquest Pro 12 (Asahi, Japan) was then taken over a micro catheter using a parallel wire strategy and successfully negotiated in distal true lumen of LAD (T2). After pre dilatation of LAD, Conquest Pro wire was exchanged for a floppy guide wire over a micro-catheter. IVUS run was then taken from LAD to LM and LCx to LM for vessel sizing. In view of the discrepancy in size of LAD/LCx and LM, 2 coronary stents were placed in a V technique from LM to LAD and LM to LCx and deployed. The stents were then post dilated and final kissing balloon inflation was done and the results were optimised by IVUS. Final cine showed well expanded LM LAD/LCx stents with TIMI 3 flow (T3).

Case Summary
This was a challenging case of long segment ostial LAD CTO with ambiguous stump.