CASE20250821_010
PCI in a STEMI Patient With Severe Kyphoscoliosis, Dextrorotation of Heart of Heart, Infrarenal Aortic Occlusion & Difficult Radial Access
By Thomas George
Presenter
Thomas George
Authors
Thomas George1
Affiliation
Caritas heart institute, India1
View Study Report
CASE20250821_010
ACS/AMI - ACS/AMI
PCI in a STEMI Patient With Severe Kyphoscoliosis, Dextrorotation of Heart of Heart, Infrarenal Aortic Occlusion & Difficult Radial Access
Thomas George1
Caritas heart institute, India1
Clinical Information
Relevant Clinical History and Physical Exam
60 year old male hypertensive presented with intermittent left-sided chest pain for 2-3 days, increasing intensity on the day of admission. There was no prior diabetes. He was a non-smoker and worked as a bartender. On examination, he had severe kyphoscoliosis with a barrel chest. Lower limb pulsations were feeble with some evidence of atrophy in the calf muscles. His blood pressure was 160/80mmHg in the right upper limb. Heart sounds were faintly heard and air entry was equal bilaterally.
 SHIBU V J_(S9_F1-91).mp4
SHIBU V J_(S9_F1-91).mp4
SHIBU V J_(S23_F1-20).mp4
Relevant Test Results Prior to Catheterization
ECG showed sinus rhythm and ST elevation from V1-V5. Echo: anterior wall RWMA, moderate LV dysfunction. Creatinine: 0.8. RBS: 113mg/dL. Hb:10.2g/dL.
Relevant Catheterization Findings
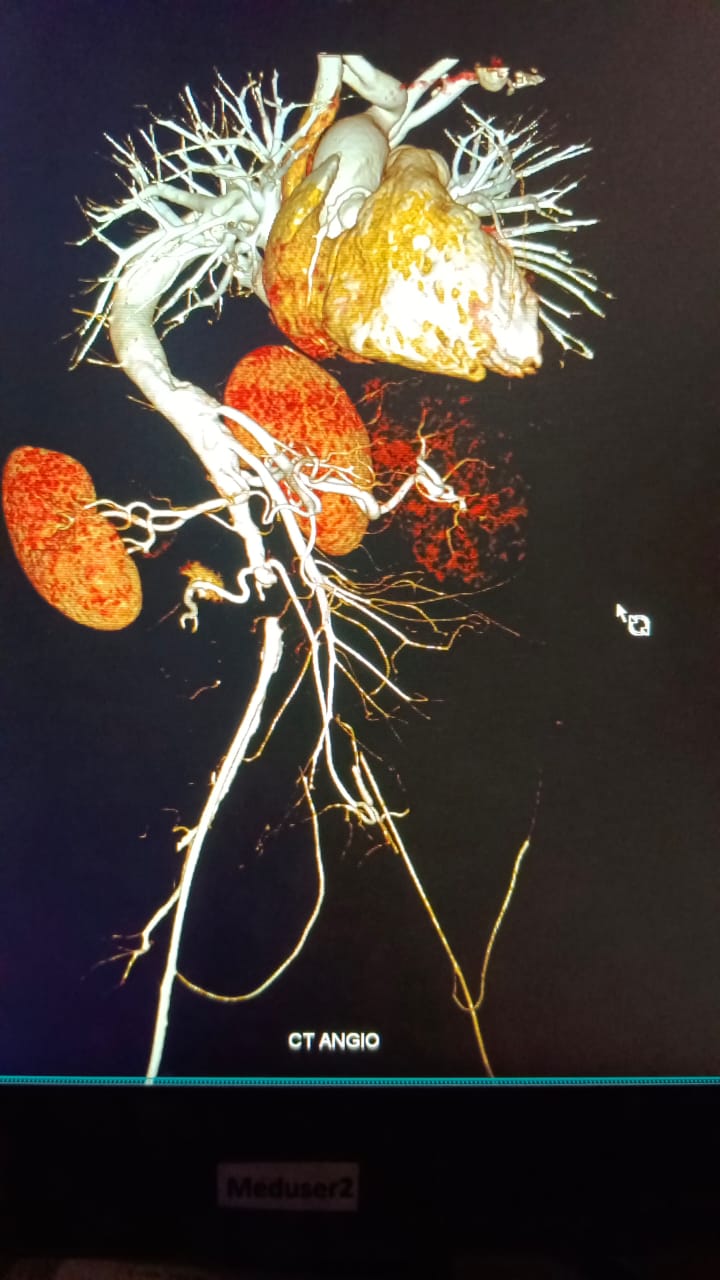
Access was right radial. It was difficult to cannulate the coronaries due to extreme kyphoscoliosis and dextroposition of the heart. Right femoral access was taken. As the teflon wire was not able to cross beyond the bifurcation of the aorta, we took a check angiogram which showed infrarenal abdominal aortic occlusion. Left main was normal. LAD mid segment was totally occluded. LCX-mild proximal disease. Proximal to mid RCA-70-80% stenosis.
SHIBU V J_(S14_F1-34).mp4
SHIBU V J_(S18_F1-330).mp4
SHIBU V J_(S24_F1-72).mp4
Interventional Management
Procedural Step
LMCA cannulated. Right radial access. 6F EBU 3.0 guide catheter. Both LAD and diagonal wired with 0.014 run-through wire. LAD pre-dilated with 2.25 x 15 NC balloon at 12atm. LAD stented with 2.25 x 44 Ultimaster Nagomi at 14atm. Post-dilated with 3 x 15 NC balloon at 20atm. Intracoronary vasodilators given. TIMI 3 flow. RCA cannulated with 6F JR3 guide catheter right radial access. RCA lesion crossed with run-through wire and pre-dilated with 25 x 15 NC balloon at 12atm. Proximal to mid RCA stented with Ultimaster Nagomi 2.75 x 44 at 14 atm. Post-dilated with 3 x 15 NC balloon at 20 atm. TIMI 3 flow.
SHIBU V J_(S22_F1-60).mp4
SHIBU V J_(S27_F1-47).mp4
SHIBU V J_(S13_F1-45).mp4
Case Summary
Deformities of the spine and thoracic cage in kyphoscoliosis can cause distortion of cardiac silhouette & coronary interventions become challenging due to the unfavorable anatomy of the aortic arch and difficulty to make the guide catheters co-axial. In this case we had to wire both LAD and diagonal through a non-coaxial guide catheter and then realign it to make it coaxial. The kinking /twisting of the aorta made this difficult. The procedure had to be completed quickly as the patient was had anterior wall STEMI. We achieved good results and after a week we did PCI to the RCA lesion . We present this case as an interesting and challenging case due to unfavourable aortic anatomy