CASE20250822_001
A Case of Protruding Stent at the Right Coronary Ostium: Rewiring by the Tip Detection Method and Adjustment With the Stent Push Technique Using a Large Balloon
By Yoshitomo Tsutsui, Yuta Nishimura, Kiwamu Sudou, Kota Tanaka, Masakazu Yasuda, Tomohiro Yamasaki, Satoshi Watanabe, Mutsumi Iwamoto, Yasushi Koyama, Atsunori Okamura, Heitaro Watanabe
Presenter
Yoshitomo Tsutsui
Authors
Yoshitomo Tsutsui1, Yuta Nishimura1, Kiwamu Sudou1, Kota Tanaka1, Masakazu Yasuda1, Tomohiro Yamasaki1, Satoshi Watanabe1, Mutsumi Iwamoto1, Yasushi Koyama1, Atsunori Okamura1, Heitaro Watanabe1
Affiliation
Sakurabashi Watanabe Advanced Health Hospital, Japan1
View Study Report
CASE20250822_001
Adjunctive Procedures - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
A Case of Protruding Stent at the Right Coronary Ostium: Rewiring by the Tip Detection Method and Adjustment With the Stent Push Technique Using a Large Balloon
Yoshitomo Tsutsui1, Yuta Nishimura1, Kiwamu Sudou1, Kota Tanaka1, Masakazu Yasuda1, Tomohiro Yamasaki1, Satoshi Watanabe1, Mutsumi Iwamoto1, Yasushi Koyama1, Atsunori Okamura1, Heitaro Watanabe1
Sakurabashi Watanabe Advanced Health Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
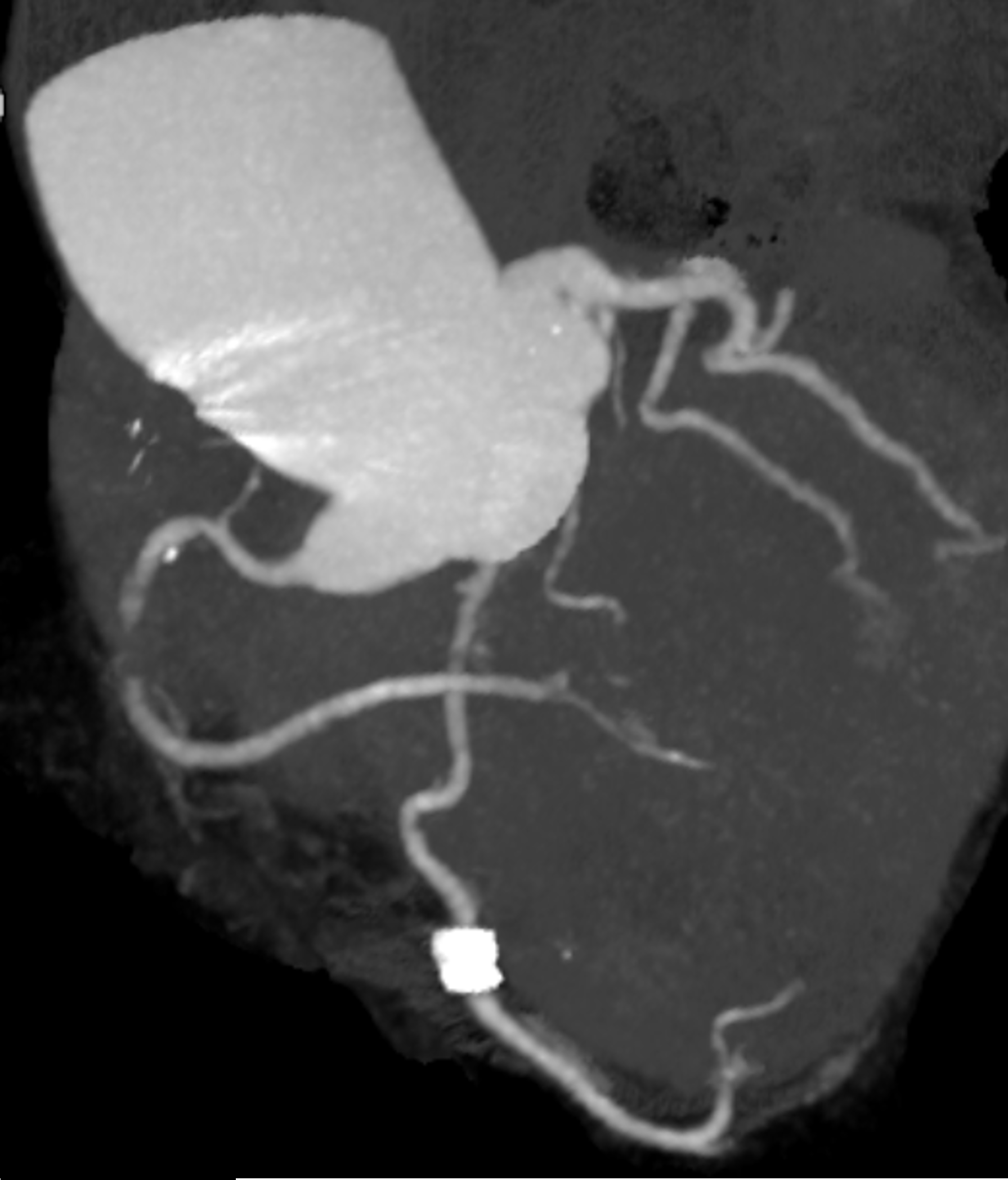
The patient was an 80-year-old woman with ahypertension, dyslipidemia, and permanent pacemaker implantation for completeatrioventricular block. She presented to another hospital with resting chestpain. The coronary computed tomography revealed severe stenosis or occlusion inthe right coronary artery (RCA), and she was referred to our hospital with adiagnosis of unstable angina.
Relevant Test Results Prior to Catheterization
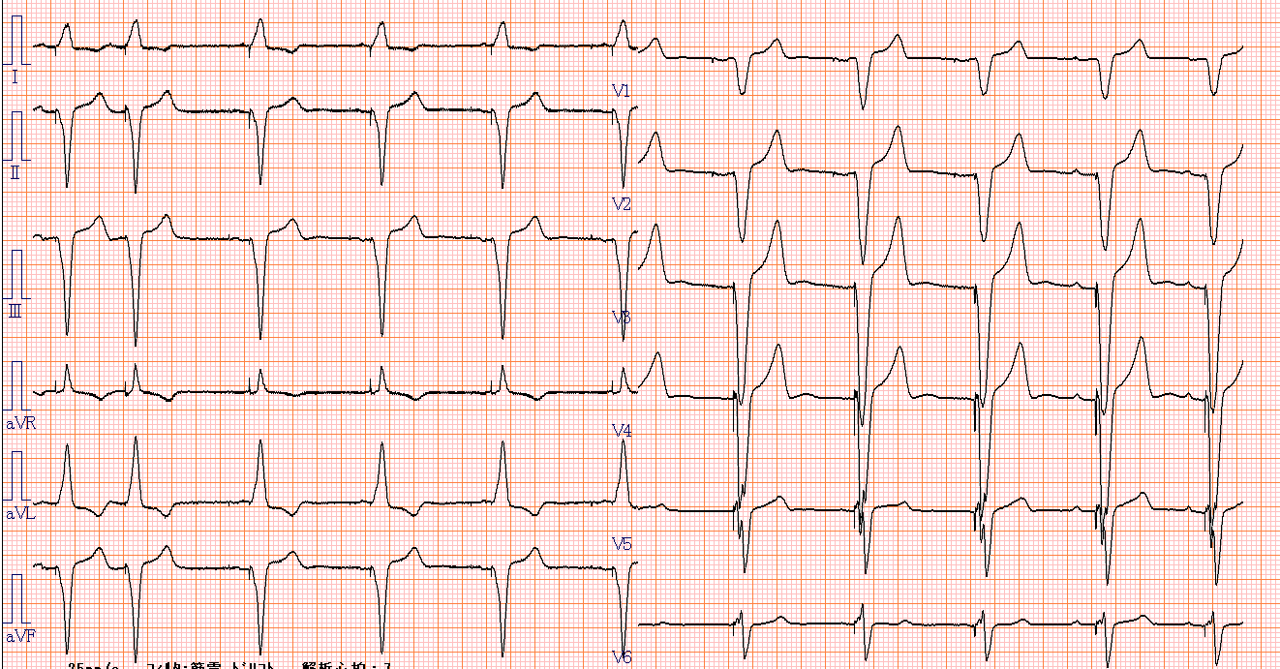
The electrocardiogram showed complete rightventricular pacing, making ST-segment changes unclear. Cardiac enzymes such astroponin T or creatine kinase were within normal limits. The echocardiography revealedleft ventricular wall motion abnormalities in the inferior wall, but global leftventricular systolic function was preserved.
Relevant Catheterization Findings
An urgent coronary angiography showed an occlusionin the middle-part of the RCA. Rentrop grade 3 collateral arteries from theleft coronary artery to the distal RCA were observed.
 CAGRCA.mp4
CAGRCA.mp4
CAGLCA.mp4
Interventional Management
Procedural Step
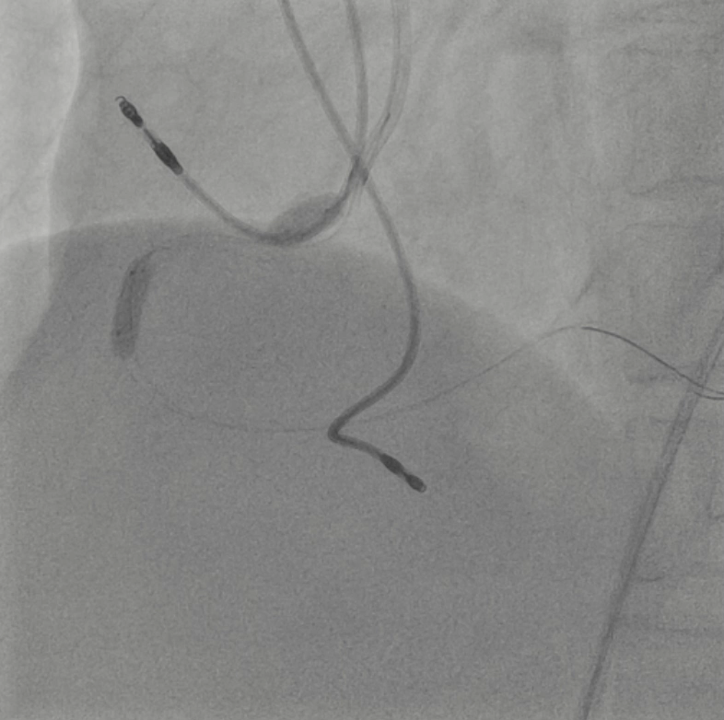
A 7Fr guiding catheter (GC) was insertedvia the right femoral artery. The lesion was crossed using a floppy wire, and intravascularultrasound (IVUS) revealed a severe stenosis caused by a non-calcified plaque.The lesion was dilated using a scoring balloon. Subsequent IVUS showed an intimaldissection at the RCA ostium. To cover the initial dissection, a drug-elutingstent was deployed from the RCA ostium, followed by post-dilation with a 3.75mmnon-compliant balloon (NCB) inside the stent. IVUS demonstrated proximal stentelongation with approximately 5 mm aortic protrusion from the RCA ostium. Stentpush from the aorta using a 5.0 mm NCB, however, the GC was crushed due toinsufficient backup support. The recrossed wire passed through the side of thestent struts, and even with the knuckle wire technique, it could not beadvanced through the central lumen of the stent. IVUS was advanced thorough thiswire, and another floppy wire was successfully reinserted into the stent fromthe stent edge using the tip detection method. Another wire was placed in theRCA using a double-lumen catheter, and the anchor balloon technique wasperformed in the middle-part of the RCA with a 3.75mm NCB. Then, the stent pushtechnique was performed using a 5.0 mm NCB to shorten the elongated stent,followed by post-dilation of the proximal stent with the 3.75mm NCB. IVUSconfirmed successful stent shortening, with approximately 1.2mm of stentprotrusion into the aorta, which was acceptable.
7.MPG
final.mp4
Case Summary
We report a case of protruding stent at theright coronary ostium that was rewired by the tip detection method and adjustedwith the stent push technique using a large balloon. The IVUS-guided tipdetection method was useful for guiding the wire into the inside of the stent.Accurate positioning of aorto-ostial coronary stents is technically difficult,so it is sometimes unavoidable for stent protrusion. However, stent pushtechnique can be an effective method for adjusting stent protrusion to theaorta.