CASE20250822_002
From Coronary Artery to Renal Artery: Successful Retrieval of a Dislodged Stent With a Homemade Device
By Deddy Hermawan Susanto, Chevanka Ursula Ayunindya, Antonia Anna Lukito
Presenter
Deddy Hermawan Susanto
Authors
Deddy Hermawan Susanto1, Chevanka Ursula Ayunindya1, Antonia Anna Lukito1
Affiliation
Siloam Hospital Lippo Village, Indonesia1
View Study Report
CASE20250822_002
Complication Management - Complication Management
From Coronary Artery to Renal Artery: Successful Retrieval of a Dislodged Stent With a Homemade Device
Deddy Hermawan Susanto1, Chevanka Ursula Ayunindya1, Antonia Anna Lukito1
Siloam Hospital Lippo Village, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 54-year-old male presented to the emergency department with an 8-hour history of typical chest pain, described as a heavy pressure over the left chest radiating to the left arm and back, accompanied by diaphoresis and nausea. His cardiovascular risk factors included hypertension and active smoking, with no prior history of CAD. On examination, blood pressure was elevated at 155/90 mmHg, with no cardiac murmurs, pulmonary crackles, or clinical evidence of heart failure (Killip class I).
Relevant Test Results Prior to Catheterization
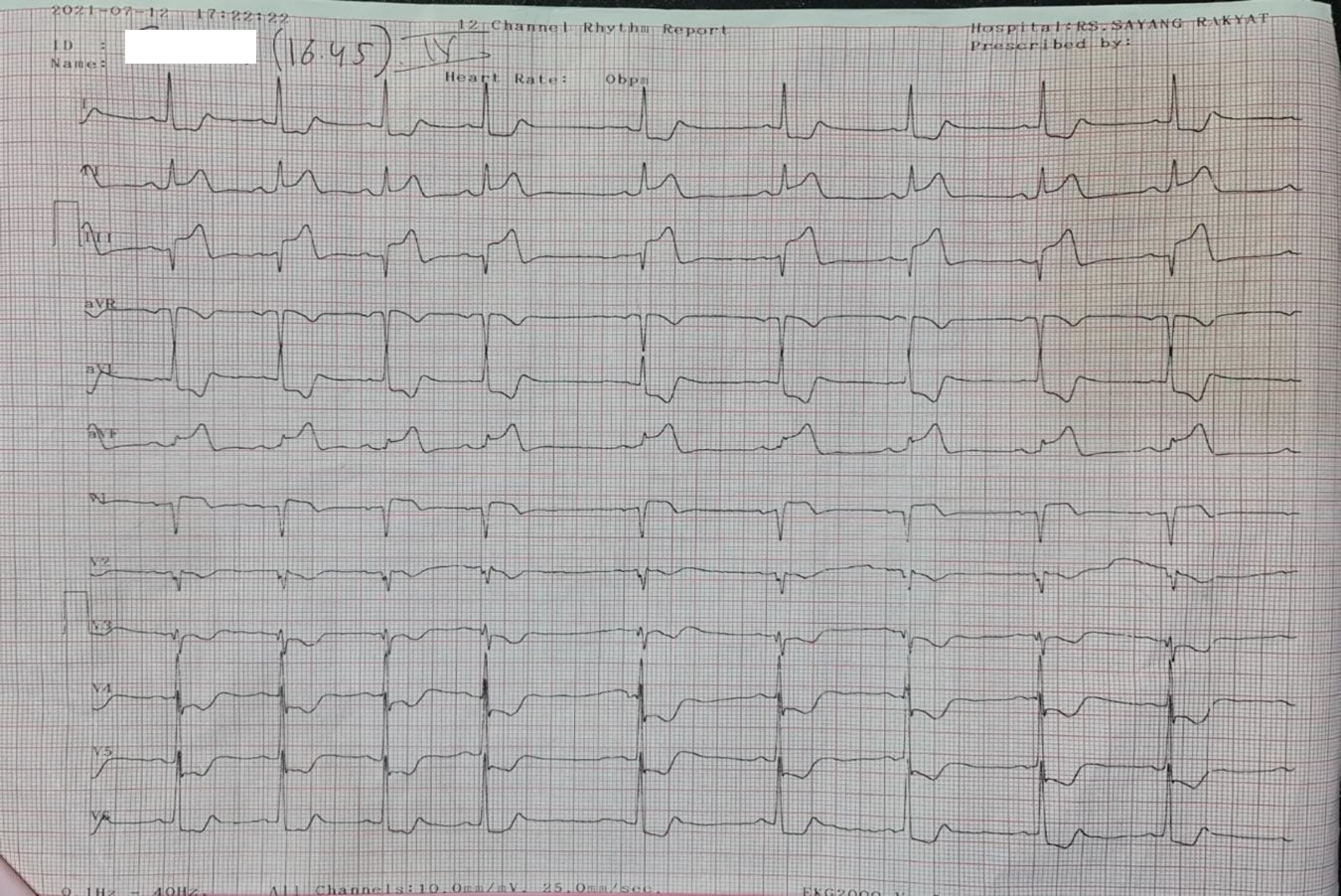
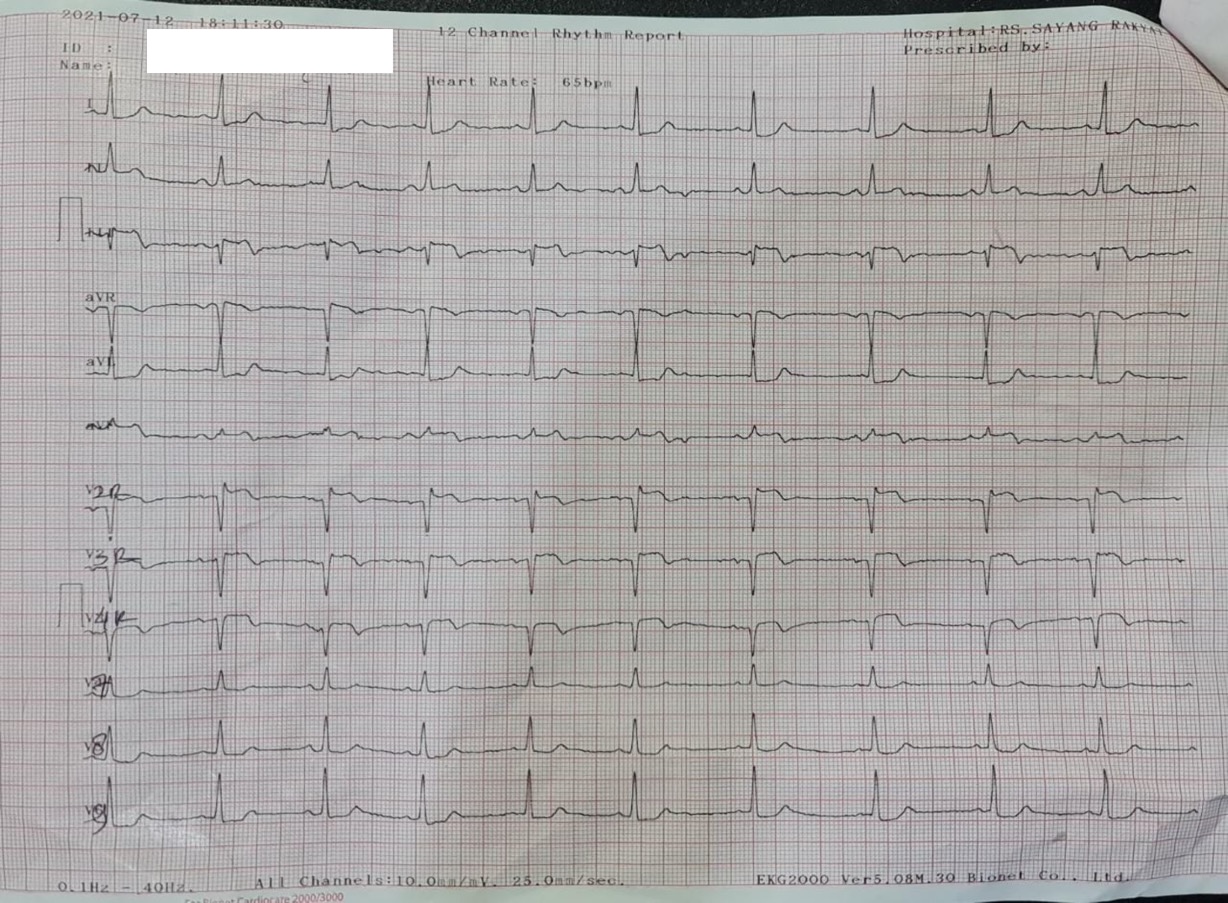
Electrocardiography demonstrated sinus rhythm with ST-segment elevation in leads II, III, aVF, and right-sided precordial leads (V3R–V4R), with reciprocal ST-segment depression in leads I, aVL, and V5–V6, consistent with acute inferior wall myocardial infarction with right ventricular involvement. Initial laboratory testing revealed elevated high-sensitivity troponin T.
Relevant Catheterization Findings
Coronary angiography was initially performed via the right radial artery using a 5Fr diagnostic catheter, which revealed subtotal stenosis of the proximal–mid left anterior descending (LAD) artery, 70% stenosis of the distal left circumflex (LCx) artery, and subtotal stenosis of the mid right coronary artery (RCA) with hazy thrombus. The culprit lesion was identified as the RCA.
 CAG LCx.mp4
CAG LCx.mp4
CAG LAD.mp4
CAG RCA.mp4
Interventional Management
Procedural Step
Primary PCI was performed using a JR 3.5/6 Fr guiding catheter. Predilatation was achieved with Sapphire III balloons (OrbusNeich, Shenzhen) 2.0 × 15 mm and 2.5 × 15 mm, both at 14 atm. Advancement of a 3.5 × 34 mm Resolute Integrity drug-eluting stent (Medtronic) to the proximal-mid RCA was unsuccessful, likely due to a calcified nodule. During attempted withdrawal, patient coughing caused guiding catheter disengagement and stent dislodgement. Initial retrieval using the multiwire technique failed, and the stent migrated into the ascending aorta. Further attempts with repeated snaring using a Goose Neck catheter, and multiwire entanglement were also unsuccessful, with subsequent stent migration to the descending aorta and final lodging in the left renal artery. Given limited retrieval devices, a homemade loop snare was constructed from a catheter, balloon, and 0.014″ wire: the wire was looped and secured by inflating the balloon inside the catheter, slightly exceeding its inner diameter. Bilateral femoral access was established: the right for snare introduction and the left for contrast injection. After several maneuvers, the stent was successfully retrieved. PCI of the RCA was then resumed with the aid of a guide extension catheter, enabling successful implantation of a 3.5 × 38 mm Resolute Integrity DES in the proximal-mid RCA, followed by post-dilatation. Final angiography demonstrated optimal results with TIMI 3 flow and no dissection, thrombus, or residual stenosis.
Dislodged stent - multiple attempts at retrieval.mov
Homemade loop snare.mov
PCI RCA with guidewire extension.mov
Case Summary
Stent dislodgement is a rare but potentially life-threatening complication of PCI, associated with adverse outcomes including coronary occlusion, myocardial infarction, arrhythmias, dissection, or stent thrombosis. Migration to extracoronary sites may also result in systemic embolization, such as stroke, renal infarction, or peripheral artery occlusion. This case highlights the challenges of managing stent dislodgement and the need for prompt retrieval to prevent serious complications. The successful use of a homemade snare demonstrates an effective alternative in resource-limited settings, emphasizing the importance of adaptability and procedural innovation in interventional cardiology.