CASE20250822_005
Zero Contrast PCI by IVUS Guide for a Patient With Renal Insufficiency
By Seung-Woon Rha, Manda Satria Chesario
Presenter
Manda Satria Chesario
Authors
Seung-Woon Rha1, Manda Satria Chesario2
Affiliation
Korea University Guro Hospital, Korea (Republic of)1, Korea University Guro Hospital, Indonesia2
View Study Report
CASE20250822_005
Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Zero Contrast PCI by IVUS Guide for a Patient With Renal Insufficiency
Seung-Woon Rha1, Manda Satria Chesario2
Korea University Guro Hospital, Korea (Republic of)1, Korea University Guro Hospital, Indonesia2
Clinical Information
Relevant Clinical History and Physical Exam
A 58 years old man with diabetes and smoking as a risk factor complains of resting chest pain during his visit to outpatient department. Patient underwent CAG on December 2020. After the CAG, patient was planned to do elective PCI on lesion at OM the next month.
Relevant Test Results Prior to Catheterization
Baseline serum creatinine level before PCI was 2.08. Hence a special precautions had to be done to preserve the renal function. To overcome this situation, we did ultra low or zero contrast PCI under IVUS guidance with massive pre-and post hydration.
Relevant Catheterization Findings
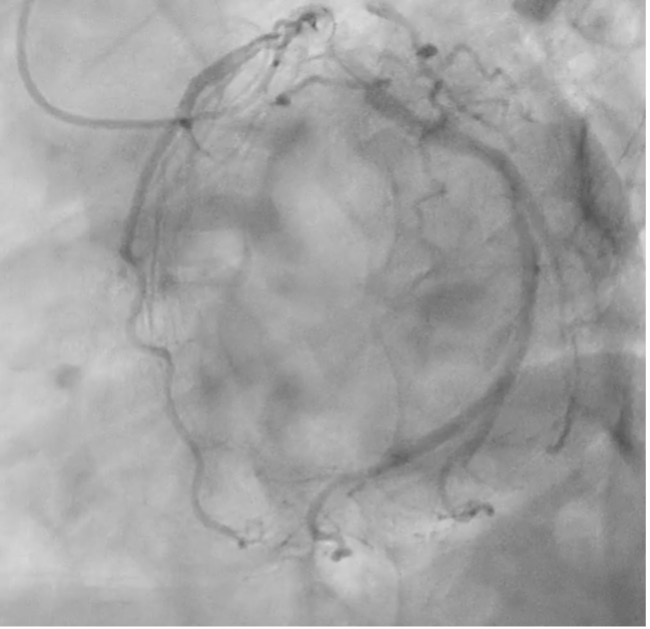
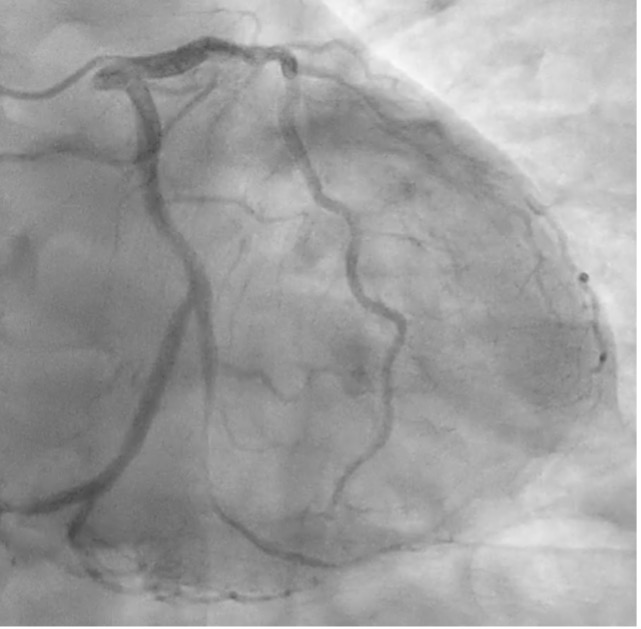
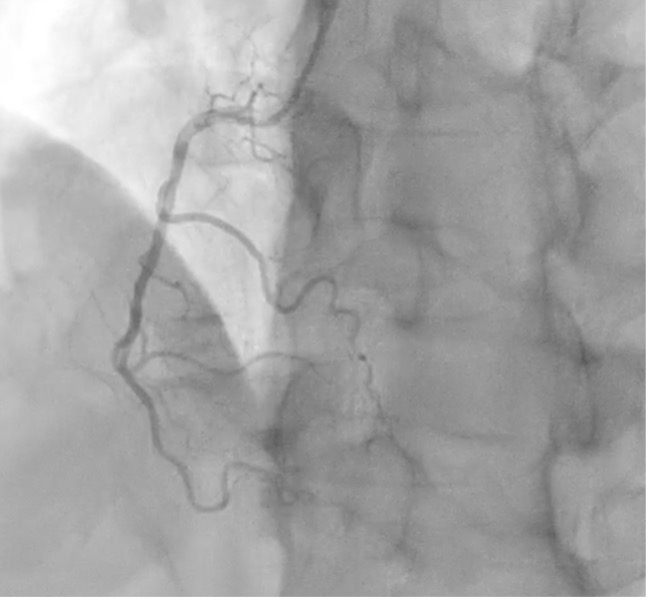
CAG shows mild diffuse stenosis at mid to distal LAD, severe diffuse stenosis at obtuse marginal, and mild diffuse stenosis at RCA (Pic 1, 2, 3).
Interventional Management
Procedural Step
Approach right radial artery, 6F EBU 3.5 SH. Sion Blue guidewire successfully advanced and into distal LCX without contrast. Second wire, the first Runthrough wire inserted into small OM branch (later it can be used as a proximal marker for stent implantation) , and the third wire, a second Runthrough wire successfully inserted into distal OM1.IVUS pre PCI was done and shown the distal reference diameter 2.5 mm and culprit lesion MLA <2.0 mm2. Lesion length approximately 35-40 mm (Video 1)Stent deployed under fluoroscopic guidance of the IVUS-marking images. Ballooning Kamui 2.0x20 mm, followed by CRE-8 stent 2.5x31 mm at distal to mid OM1 and CRE-8 2.75x16 mm from mid to proximal OM1 in overlapping method (Video 2).IVUS evaluation done and showed a satisfactory result of well apposed and fully expanded stent without complication (Video 3)To finalize the procedure, ultra low contrast with diluted saline contrast was injected to take the final angiogram. Angiogram showed no significant residual stenosis or complication with good distal run-off.
 Video 1.mp4
Video 1.mp4
Video 2.mp4
Video 3.mp4
Case Summary
All procedures were successfully completed with ultra low contrast administration. And without renal function deterioration (laboratory finding on creatinin post PCI are 2.05), pericardial effusion, or stent edge dissection.