CASE20250822_008
Intravascular Ultrasound Guided PCI for Calcified Right Coronary Artery In-Stent Restenosis: Overcoming Intravascular Lithotripsy With Rotational Atherectomy
By Zhi Yuan Loh
Presenter
Zhi Yuan Loh
Authors
Zhi Yuan Loh1
Affiliation
Cheng Hsin General Hospital, Taiwan1
View Study Report
CASE20250822_008
Complex PCI - In-Stent Restenosis
Intravascular Ultrasound Guided PCI for Calcified Right Coronary Artery In-Stent Restenosis: Overcoming Intravascular Lithotripsy With Rotational Atherectomy
Zhi Yuan Loh1
Cheng Hsin General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
This 54-year-old male with underlying history of coronary artery disease with double vessel disease, status post percutaneous coronary intervention for right coronary artery, hypertension and hyperlipidemia for years with both under medication control. He complained of intermittent chest tightness and shortness of breath for weeks with symptoms progressively worsening. Physical examinations showed clear breathings sounds, Grade I systolic murmur at apex with regular heart beats.
Relevant Test Results Prior to Catheterization
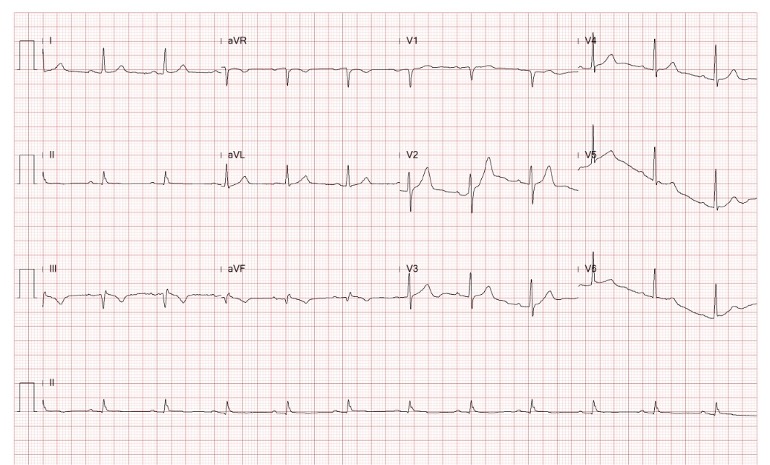
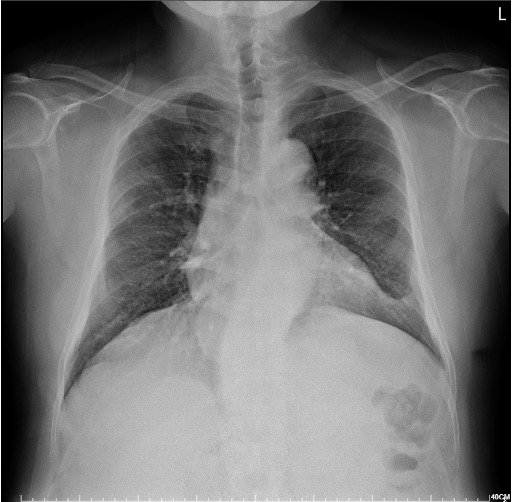
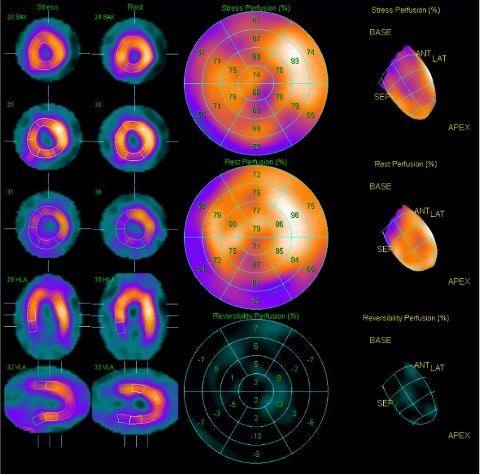
His ECG showed sinus rhythm with old inferior myocardial infarctions. CXR showed cardiomegaly otherwise unremarkable. Transthoracic echocardiography revealed preserved LV systolic function, competent valves function and LV posterior wall hypokinesis. Thallium scan revealed ischemia for left anterior descending artery and right coronary artery.
 4.mp4
4.mp4
Relevant Catheterization Findings
Coronary angiography revealed CAD-TVD with LAD-P 80% stenosis and severe calcifications, RCA-D 90% ISR and severe calcifications, LCx-M 60% stenosis and OM1 90% stenosis. LVG showed basal inferior to posterior hypokinesis.
9518929_007.mp4
9518929_010.mp4
9518929_012.mp4
Interventional Management
Procedural Step
For the index procedure, LMCA was engaged smoothly with JL3.5/7F guiding catheter. Runthrough floppy was advanced to LAD-D. IVUS showed 360 degree calcifications with proximal reference vessel diameter 4.0mm. We used 4.0x12mm IVL Shockwave C2+ to dilate LAD-P in total 30 shots. Due to dissection, a 4.0 x 24mm DES was deployed and Post-dilatation with 4.0 x 15m NC balloon. We the continued PCI for RCA-D ISR. After RCA was engaged with JL3.5/7F guiding catheter, we introduced Runthrough to PL branch smoothly. IVUS showed double-layered stents with stent underexpansion and 360 degree calcifications. We failed to advance the IVL across the ISR and it was undilatable with 4.0 x 12mm NC balloon. Despite using Guideliner/7F and POBA with IVL and NC balloon in the proximity to the ISR, IVL was still unable to advance and the ISR was still undilatable with the NC balloon. Due to prolonged procedure time, we performed staging PCI 1 month later. During the procedure, RCA was engaged smoothly with JL3.5/7F guiding catheter, we advanced IVL across the RCA-D ISR successfully after POBA with 4.0 x 15mm NC balloon, but it was still undilatable after 120 shots. We then performed Rotablation by using 1.75mm burr from 140 to 180k rpm. We were then able to fully dilate the stent with 4.0 x 15mm NC balloon and 4.0 x 30mm DCB. The final angiography result was optimal and patient had tolerated the procedure well.
9518929_093.mp4
9518929_004.mp4
9518929_002.mp4
Case Summary
Imaging guided PCI is crucial t for a double-layered stent ISR because it clarifies the underlying mechanism such as stent underexpansion, malapposition, neoatherosclerosis or multiple stent layers, which may help us choose the right strategy and modalities for plaque modification such as Atherectomy, IVL, High-pressure NC balloon angioplasty, Cutting or Scoring balloon, DCB or even another stent if it is unavoidable. We may also need to recognize that IVL is difficult to advance once beeing dilated prior crossing tight lesion due to its bulky crossing profile and limited trackability due to its stiff shaft and balloon profile.