CASE20250823_003
“Expecto Patronum”! How to Use Our Talent to Rescue Nightmare Complication During PCI - Case Share
By Chi-Yao Huang
Presenter
Chi-Yao Huang
Authors
Chi-Yao Huang1
Affiliation
Taichung Veterans General Hospital, Taiwan1
View Study Report
CASE20250823_003
Complication Management - Complication Management
“Expecto Patronum”! How to Use Our Talent to Rescue Nightmare Complication During PCI - Case Share
Chi-Yao Huang1
Taichung Veterans General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
This 81 years old man with past history of (1)Congestive heart failure (ejaction fraction 26%) (2) Coronary artery disease(CAD) s/p CAB-G in 2012 (3) Chronic kidney disease (4) type 2 DM (5)Empyema s/p therapy with stasis pleural effusion . He was just discharged from our CV ward due to acute decompensated heart failure (ADHF) c/w acute pulmonary edema. This time, he was admitted due to recurrent heart failure with elevated cardiac enzyme level suspected ADHF recurrent and NSTE-ACS.
Relevant Test Results Prior to Catheterization
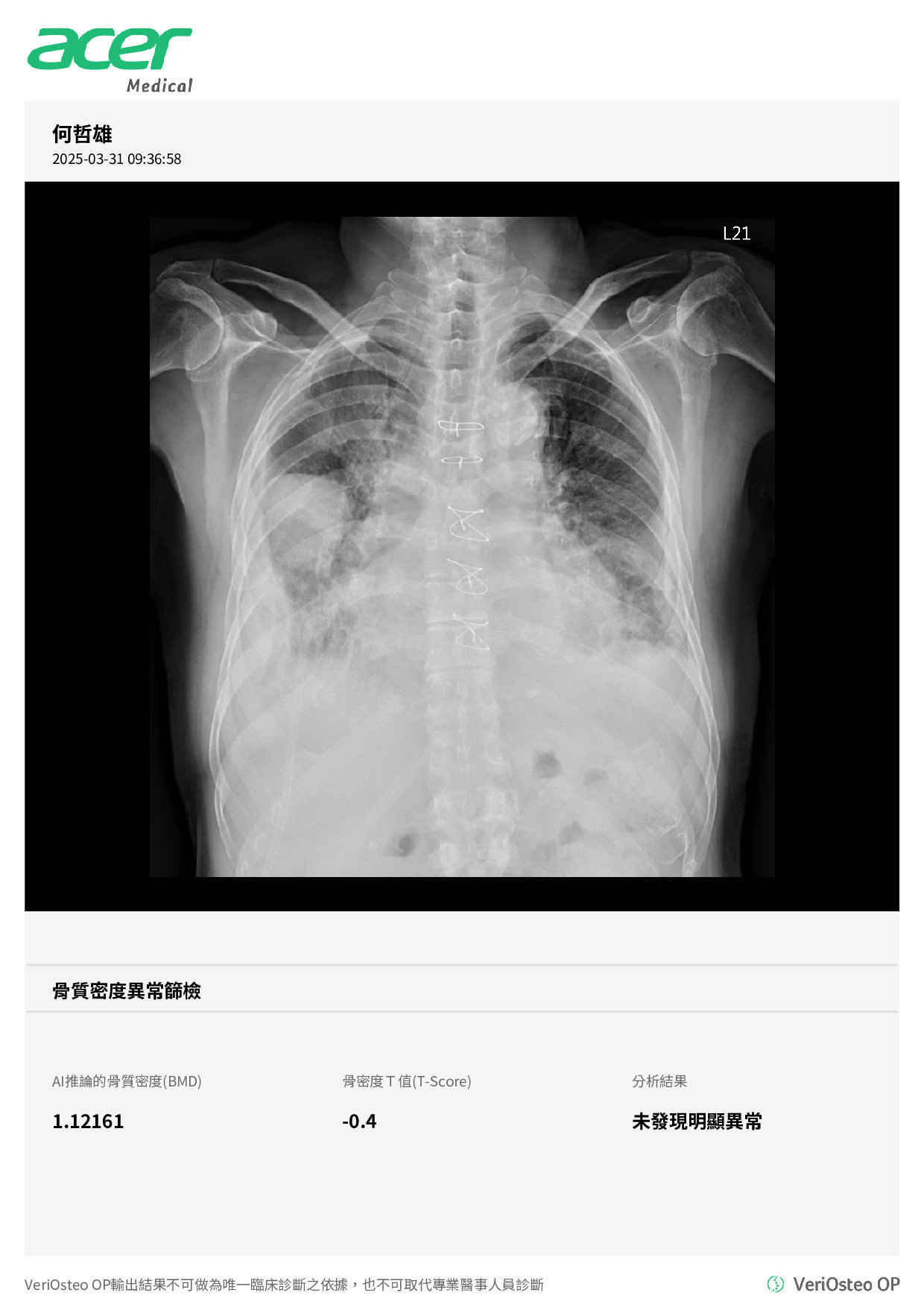
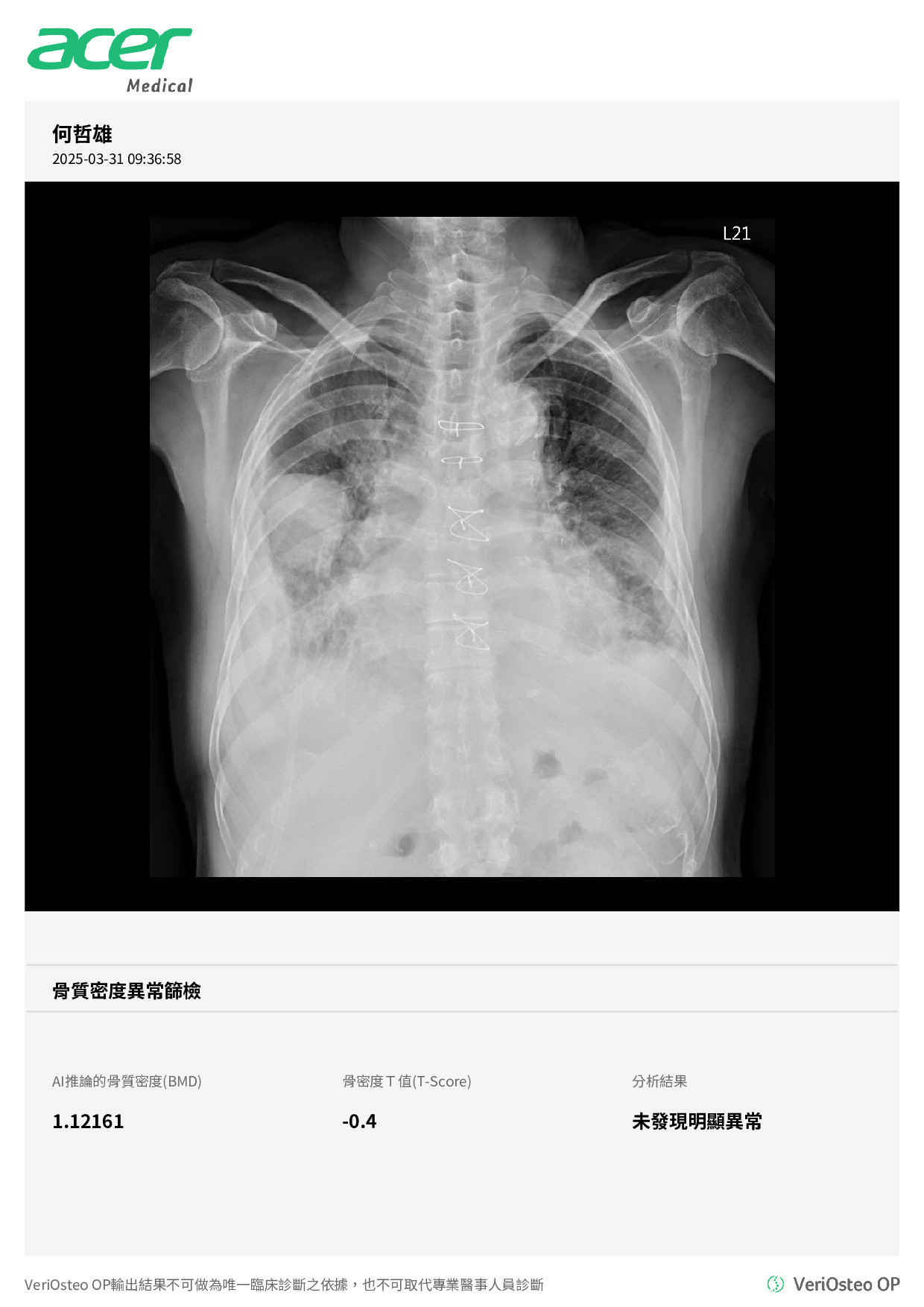
The LAB data showed elevated cardiac enzyme: CPK peak 641 CKMB 31 Troponin-T 1935, with poor renal function (eGFR around 20-30 ). CXR showed pulmonary edema, and right lower lobe stasis inter-lobar pleural effusion.
Relevant Catheterization Findings
Left Main:Diffused AS change
Left Anterior Descending:LAD CTO, DA1 diffused stenosis.
Left Circumflex:Diffused critical stenosis.
Right Coronary:RCA-P proximal segmetnal stenosis >70%RCA-M critical stenosis>90%With heavy calcified formation.Crux to PL critical stenosis> 90%with TIMI 3 flow
not done
Right Heart Catheterization:not done
Pulmonary Angiogram:not done
Other Findings:1.LIMA: showed patent
 002272549B_005.mp4
002272549B_005.mp4
002272549B_006.mp4
Left Anterior Descending:LAD CTO, DA1 diffused stenosis.
Left Circumflex:Diffused critical stenosis.
Right Coronary:RCA-P proximal segmetnal stenosis >70%RCA-M critical stenosis>90%With heavy calcified formation.Crux to PL critical stenosis> 90%with TIMI 3 flow
not done
Right Heart Catheterization:not done
Pulmonary Angiogram:not done
Other Findings:1.LIMA: showed patent
Interventional Management
Procedural Step
we used EBU 3.0x7Fr GC to engage the RCA in order to enhance the support. Then we used expressman 6.0 for better support and tried again with 2.0 mm BC and finecross that all failed to pass through the same part over the middle of the RCA. Then we decide to direct wiring the Rota wire(extrasupport). Then we successful sent the rota wire to the PL distal smoothly. Then we used a 1.25mm Burr to rota the RCA-near ostium part to RC-P (close the 1->2 part)x 3 times. But due to the large angle over 1->2, we worried about perforation and consierred to hold rotablation. However, patient complaint about chest pain and dyspena that time, the SBP was drop to 70 mmHg around. So we removed the rotablation device and do a following-up angiogrpahy showed RCA-M extravasation noted. Then we administered levophed 10ml and Protamine 0.6amp(30mg) to try to correct the active bleeding/extravasation. However, device was difficulty in going through the RCA-M part. Then we used 1.5x15mm BC, new 2.0x15mm Bc to pass through the RCA-M and successful sent the Expressman(tapper one) down to the RCA-M-D part. So we decided to deploy a DES(2.75x33mm) over the RCA-nearly ostium to RCA-PM part up to 10 bars. And then the 6Fr expressman was more easiler to pass through the RCA-M part. So we then successful sent the 6Fr expressman down to the RCA-M-D and sent the Graft stent(GRAFTMASTER STENT 2.8x16mm) to the location of extravasation site.The final result showed well expasion of the stent without more extravasation.
002272549B_028 1st run Rota.mp4
002272549B_043 A extravasation.mp4
002272549B_142 A deploy the graft stentA.mp4
Case Summary
1.While complications happened, the 1st thingto do is keeping patient’s vital signs and hemodynamic stable as possible as Ucan.