CASE20250903_002
Successful Treatment of In-Stent Restenosis of Complex Left Main Bifurcation Lesion With Reverse Crush Technique and Drug-Eluting Balloon
By Seongbong Wee
Presenter
Seongbong Wee
Authors
Seongbong Wee1
Affiliation
Asan Medical Center, Korea (Republic of)1
View Study Report
CASE20250903_002
Complex PCI - Left Main
Successful Treatment of In-Stent Restenosis of Complex Left Main Bifurcation Lesion With Reverse Crush Technique and Drug-Eluting Balloon
Seongbong Wee1
Asan Medical Center, Korea (Republic of)1
Clinical Information
Relevant Clinical History and Physical Exam
A 44-year-old male presented with worsening dyspnea on exertion for one month. He had a history of percutaneous coronary intervention (PCI) with Onyx 3.0 × 22 mm stent implantation from left main (LM) to proximal left anterior descending artery (pLAD) at another center one year prior due to LM significant stenosis.The patient presented with dyspnea on exertion consistent with NYHA class II. Physical examination was otherwise unremarkable. Electrocardiography showed normal sinus rhythm, chest X-ray revealed no significant abnormalities, and transthoracic echocardiography demonstrated normal left ventricular ejection fraction.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
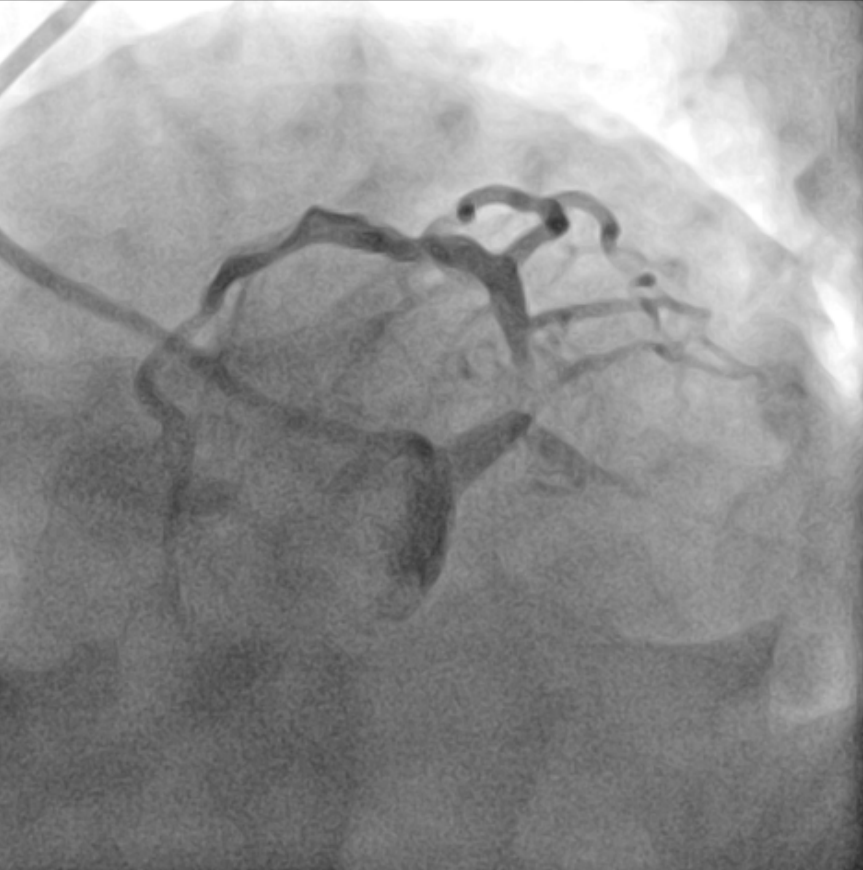
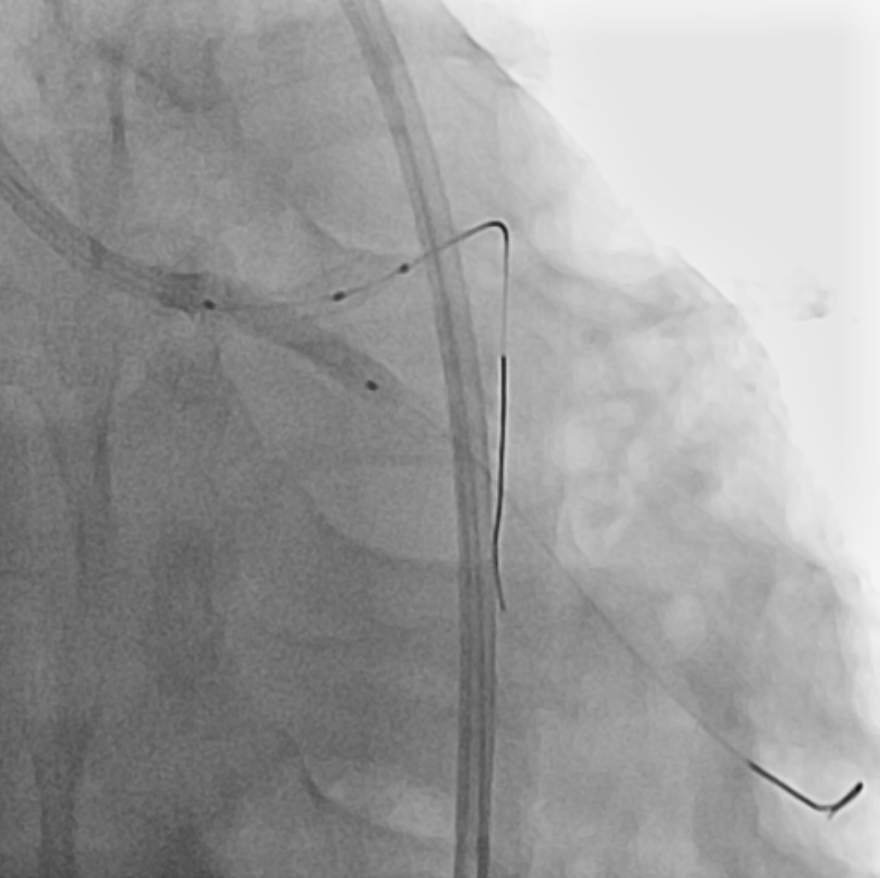
Coronary angiography revealed no specific findings in the right coronary artery, while showing collateral flow from the posterior descending artery to septal branches. Severe in-stent restenosis (ISR) was observed in the previous LM stent, accompanied by severe stenosis at the left circumflex (LCX) ostium resulting in TIMI flow grade 1.The procedure was performed via femoral approach using an 8 Fr sheath and Judkins 3.5 guiding catheter. Runthrough NS 0.014 wire was used for LAD wiring, which was successfully achieved. However, LCX wiring proved challenging and required a double lumen catheter (Asahi Sasuke 0.014, 3.2 Fr) for successful passage.Predilatation was performed using a semi-compliant balloon (Ryurei 2.0 × 15 mm) for LCX and a non-compliant balloon (Selethru NC 3.5 × 8 mm) for LM to LAD. Intravascular ultrasound (IVUS) evaluation was performed in both vessels to assess lesion characteristics. The treatment strategy involved drug-eluting balloon (DEB) therapy for LM-pLAD ISR and drug-eluting stent (DES) implantation in LCX with reverse crush technique.Additional lesion preparation was performed using a cutting balloon (Wolverine 3.5 × 10 mm) for the LM-pLAD ISR lesion. A Xience 3.0 × 15 mm stent was implanted in the proximal LCX. The LCX stent was then crushed using a non-compliant balloon (Selethru NC 3.5 × 8 mm), followed by rewiring of LCX using the double lumen catheter and Fielder FC 0.014 wire.Kissing balloon dilatation was performed with non-compliant balloons (Selethru NC 3.5 × 8 mm for LAD and 3.25 × 15 mm for LCX) at 6 atm. Subsequently, drug-eluting balloon therapy (SeQuent Please Neo 3.5 × 20 mm) was applied to the LM-pLAD ISR lesion, followed by final kissing balloon dilatation at 8 atm.Final IVUS evaluation confirmed optimal results in both LAD and LCX vessels. The procedure was completed without complications, demonstrating successful treatment of complex left main bifurcation disease with combined DEB and reverse crush stenting technique.
Case Summary
This case highlights the effectiveness of combining drug-eluting balloon therapy for in-stent restenosis with reverse crush stenting technique in treating complex left main bifurcation lesions, achieving excellent angiographic and intravascular imaging outcomes.