CASE20250924_001
The Calcium Conquered: Upfront Rotatripsy in a Challenging LM Bifurcation Disease
By Ju Hyeon Kim, Eman Murad
Presenter
Eman Murad
Authors
Ju Hyeon Kim1, Eman Murad1
Affiliation
Asan Medical Center, Korea (Republic of)1
View Study Report
CASE20250924_001
Complex PCI - Calcified Lesion
The Calcium Conquered: Upfront Rotatripsy in a Challenging LM Bifurcation Disease
Ju Hyeon Kim1, Eman Murad1
Asan Medical Center, Korea (Republic of)1
Clinical Information
Relevant Clinical History and Physical Exam
A 73-year-old man with diabetes, hypertension, dyslipidemia, and a history of smoking presented with ongoing chest pain. He was referred after emergent angiography at an outside hospital revealed a severely calcified left main bifurcation disease with subtotal proximal LCx stenosis (Medina 1,1,1) and a SYNTAX score of 27.


Relevant Test Results Prior to Catheterization
Baseline laboratory findings were unremarkable except for mild dyslipidemia. ECG showed non-specific ST-T changes. Echocardiography demonstrated preserved LV systolic function without regional wall motion abnormalities.
Relevant Catheterization Findings
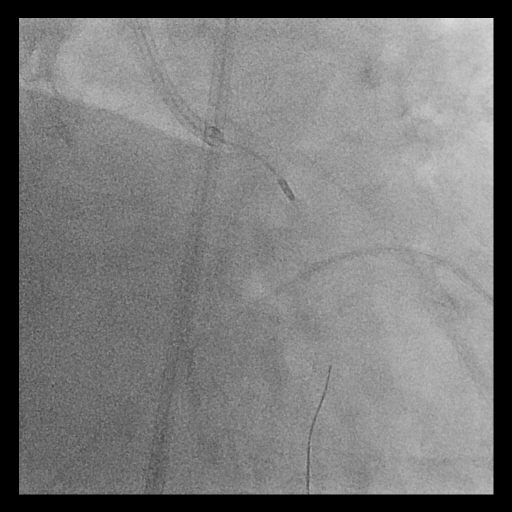
Coronary angiography showed long, tram-track dense calcification involving the left main bifurcation with subtotal occlusion of proximal LCx and diffuse proximal LAD disease. The calcified plaque exhibited significant radiopacities visible before contrast injection, suggesting a deep concentric calcium burden.
 4-1.avi
4-1.avi
Interventional Management
Procedural Step
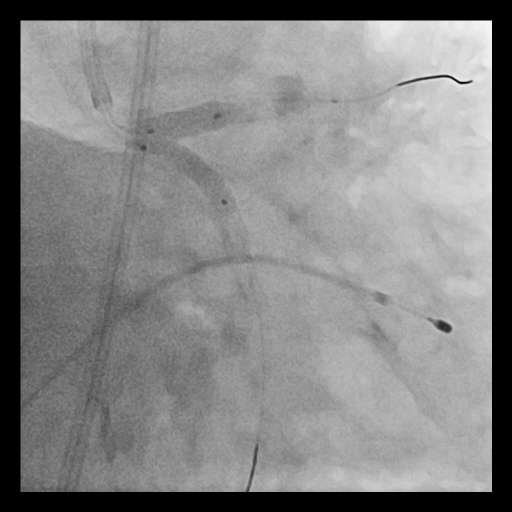
Given the extensive and concentric calcium across the LM bifurcation, an upfront “Rotatripsy” strategy (rotational atherectomy followed by intravascular lithotripsy) was selected. A 1.25 mm burr was used for initial channel creation in the LCx and LM-LAD, with transient bradycardia requiring temporary pacing. Post-rotablation IVUS revealed residual deep calcium. Subsequently, intravascular lithotripsy (IVL) using a 3.5–4.0 mm balloon (1:1 sizing to proximal LCx and LM) was applied with 8 cycles, achieving clear calcium fracture on IVUS. Two DES were implanted sequentially (LCx: 3.5×28 mm; LM–LAD: 4.0×38 mm), followed by high-pressure post-dilation and final kissing balloon inflation. Final IVUS confirmed optimal stent expansion (MSA: LCx 7.7 mm², LAD 12.1 mm², LM 13.2 mm²) and well-apposed stents throughout the bifurcation.
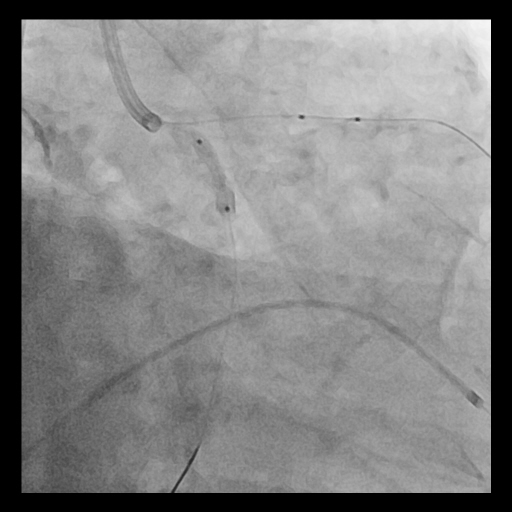
5-3.avi
5-4.avi

Case Summary
Upfront Rotatripsy combining rotational atherectomy and intravascular lithotripsy can effectively manage severely calcified LM bifurcation lesions. Intracoronary imaging is essential for understanding calcium morphology and guiding appropriate modification strategy. The hybrid approach ensures both superficial debulking and deep calcium fracture, achieving predictable stent expansion and durable results.