
CASE20210725_003
Is it Pan-Coronary Vulnerability?
By
Presenter
Ahmed Kasem
Authors
1
Affiliation
, Saudi Arabia1
Complex PCI - Multi-Vessel Disease
Is it Pan-Coronary Vulnerability?
1
, Saudi Arabia1
Clinical Information
Patient initials or Identifier Number
AA
Relevant Clinical History and Physical Exam
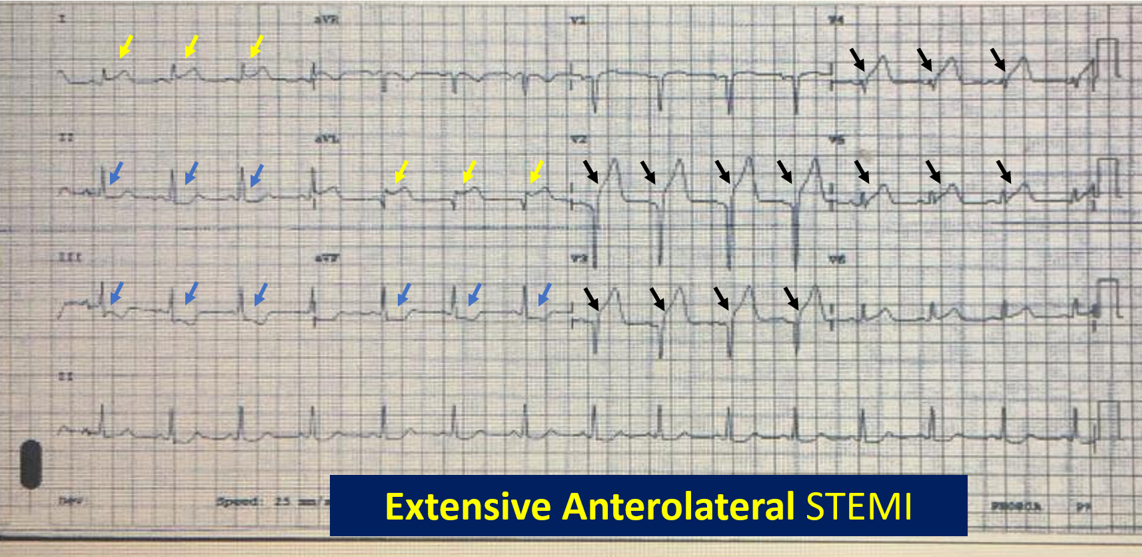
31 y/o Egyptian male patient with Known h/o heavy cig. Smoker 15 years ago, dyslipidemia. He presented to ER. troponin mold elevated, ECG showed S-T elevation in antro-lateral leads with depression in A, aVL
Relevant Test Results Prior to Catheterization
Troponin test: 0.41 on admission. ECG showed anterolateral STEMI.
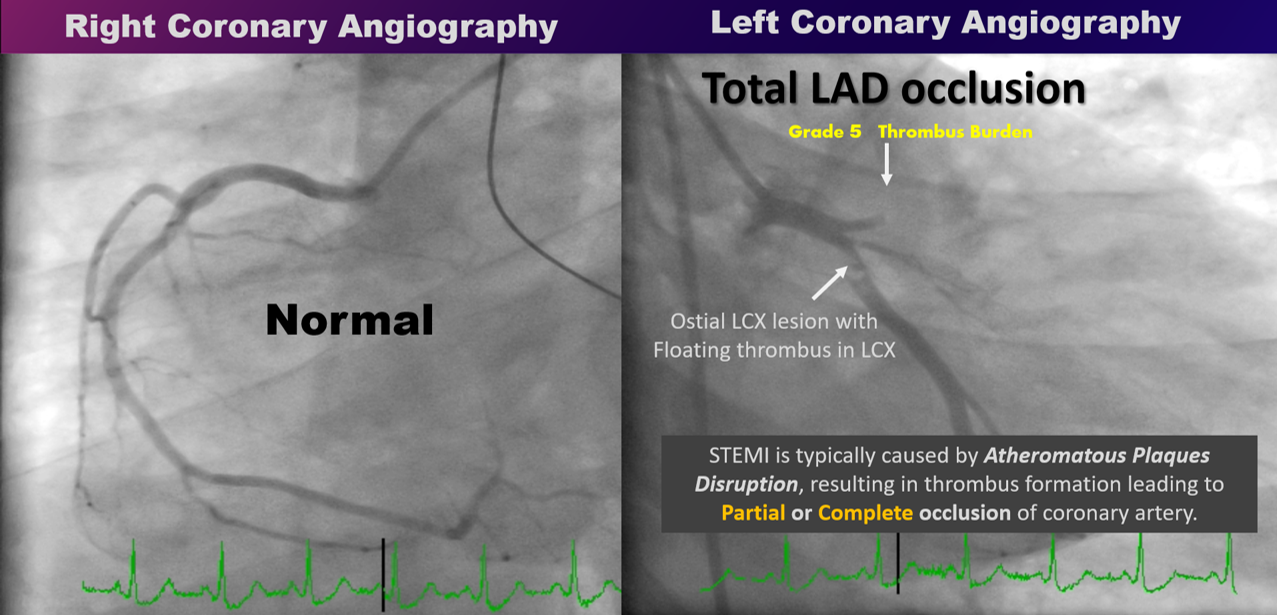
Relevant Catheterization Findings
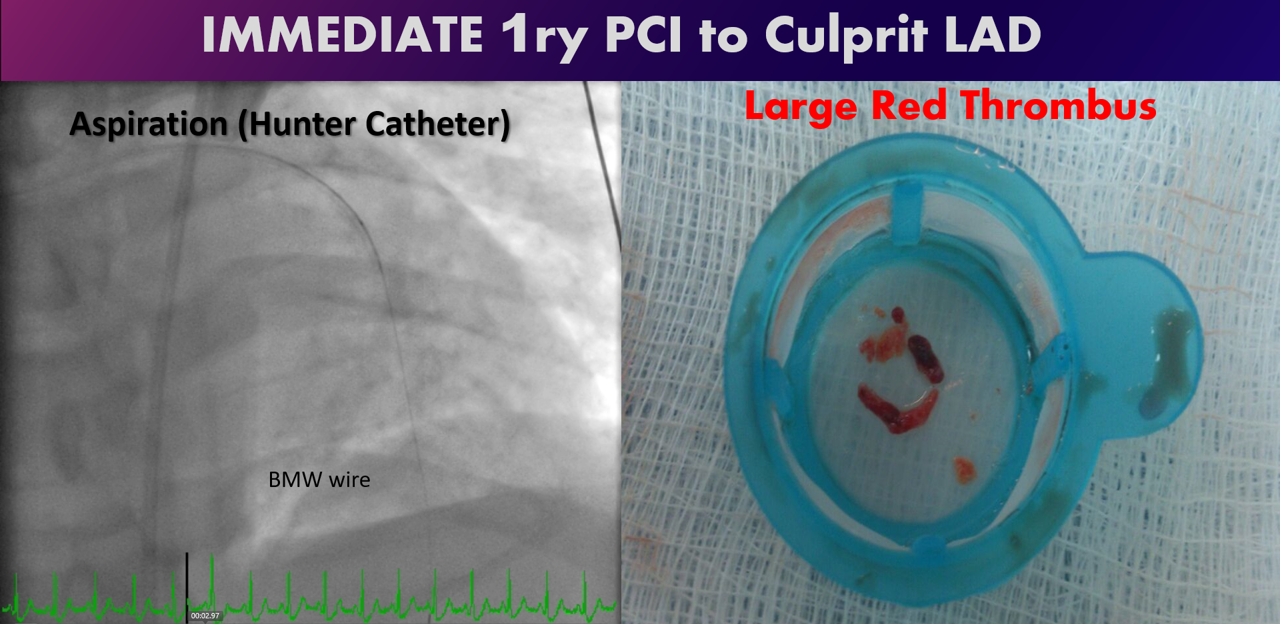
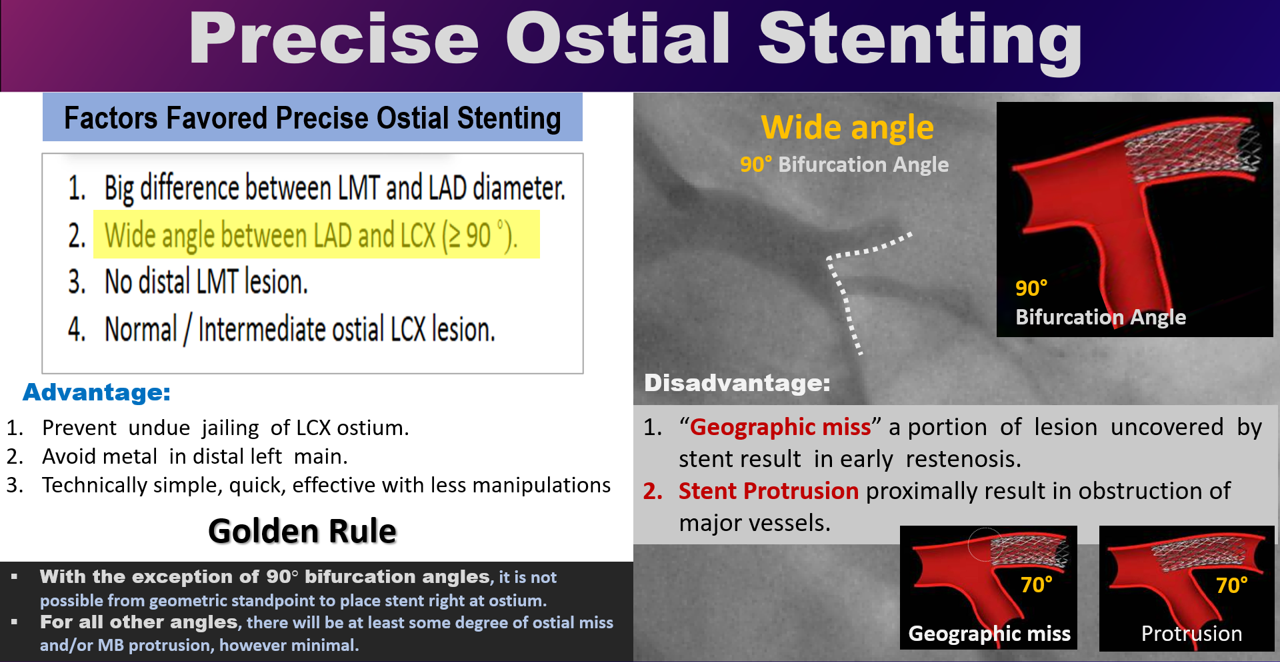
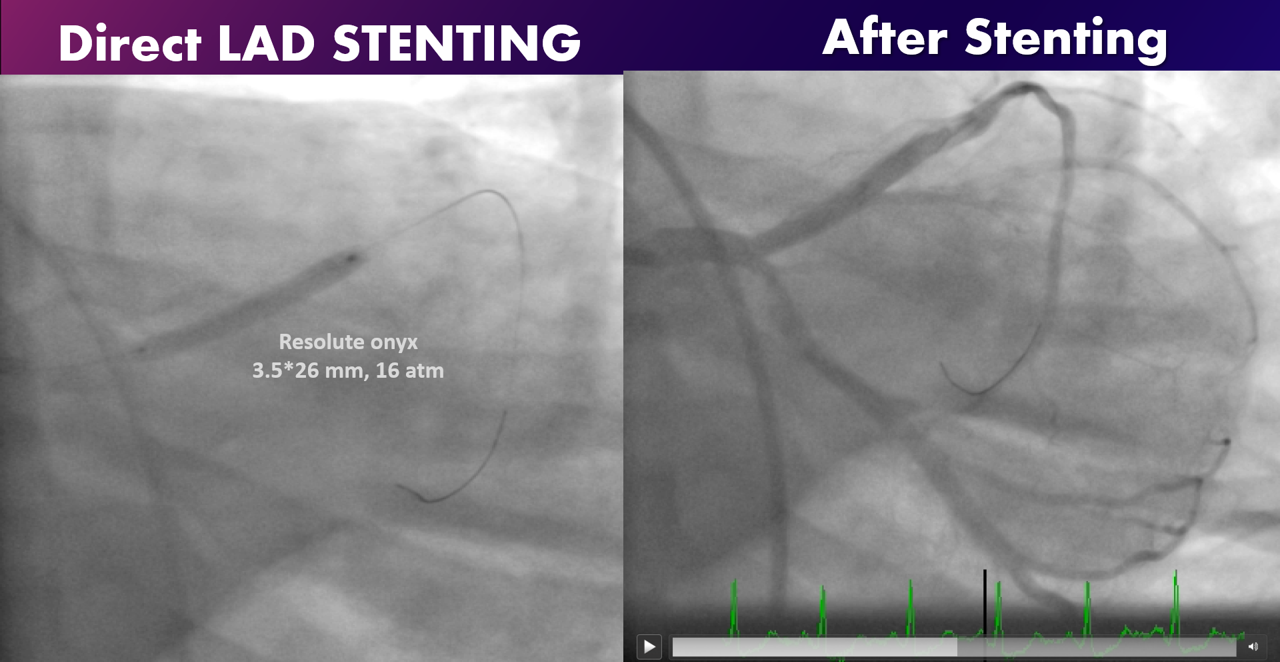
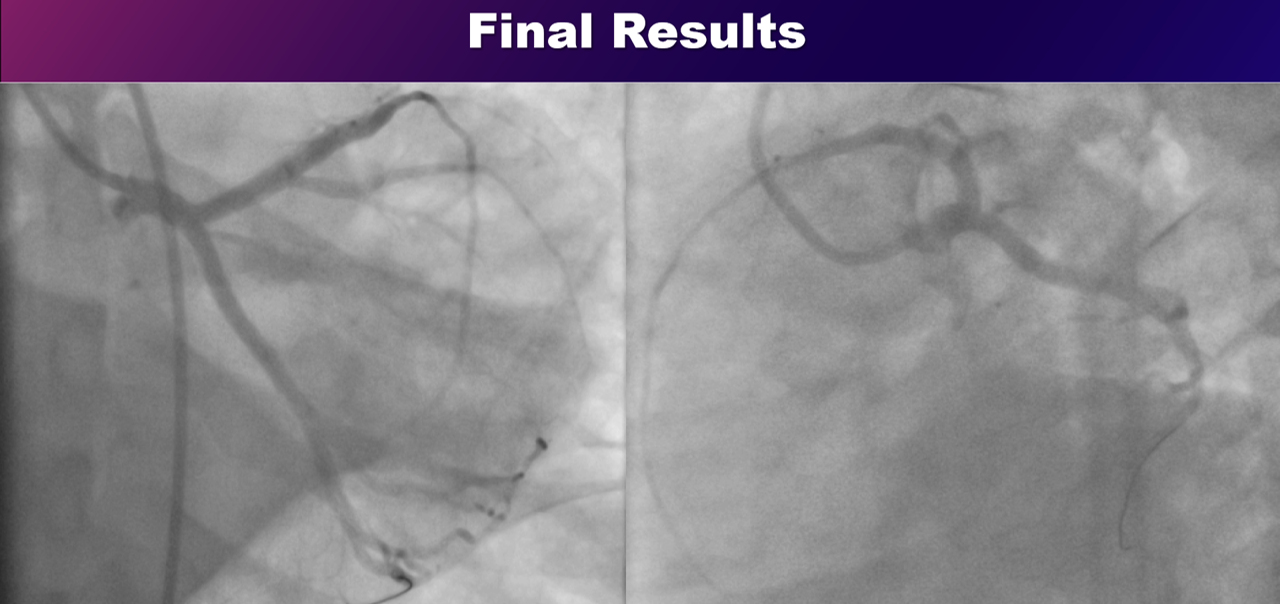
He was transferred to Cath lab for primary PCI. Coronary angiography showed: no significant disease in RCA while, LAD was total proximal occlusion and LCX was subtotal ostial occlusion with floating thrombus. Immediately BMW wire passed to LAD then aspiration thrombectomy by export Cath where only TIMI 1 flow resumed but the patient suddenly developed VF where DC shock given once and revived to sinus rhythm, then IC vasodilators was given distal IC improving the flow into TIMI 3 flow. Then DES was deployed precisely into the ostium of LAD. The question was about LCX? is it a second culprit? So we decided to deploy direct stenting to ostial LCX in V stenting like technique with excellent final results.
Interventional Management
Procedural Step
He was transferred to Cath lab for primary PCI. Coronary angiography showed: no significant disease in RCA while, LAD was total proximal occlusion and LCX was subtotal ostial occlusion with floating thrombus. Immediately BMW wire passed to LAD then aspiration thrombectomy by export Cath where only TIMI 1 flow resumed but the patient suddenly developed VF where DC shock given once and revived to sinus rhythm, then IC vasodilators was given distal IC improving the flow into TIMI 3 flow. Then DES was deployed precisely into the ostium of LAD. The question was about LCX? is it a second culprit? So we decided to deploy direct stenting to ostial LCX in V stenting like technique with excellent final results.
Case Summary
Conclusion: Pan-Coronary Vulnerability is a rare under-recognized entity only diagnosed during primary PCI as a simultaneous multi-vessel coronary thrombosis. Pan-coronary Vulnerability is a high risk group of patient presented as STEMI with severe clinical instability (Acute heart failure or Pulmonary edema, Cardiogenic shock, even sudden death from life-threatening ventricular arrhythmia (VF)). It has a very poor prognosis and higher mortality risk if not early recognized with timely and efficiently managed. Early prediction of the diagnosis is crucial (high clinical suspension, proper analysis of both ECG (STEMI localization) and echocardiography (SWMA)) to facilitate the early recognition.