
CASE20210729_001
Bail-Out Intravascular Ultrasound-Optimized Percutaneous Coronary Intervention of the Left Anterior Descending Artery Using Sasuke Double Lumen Catheter
By , , ,
Presenter
Kristy Garganera
Authors
1, 1, 1, 1
Affiliation
, Philippines1
Complications - Complications
Bail-Out Intravascular Ultrasound-Optimized Percutaneous Coronary Intervention of the Left Anterior Descending Artery Using Sasuke Double Lumen Catheter
1, 1, 1, 1
, Philippines1
Clinical Information
Patient initials or Identifier Number
FV
Relevant Clinical History and Physical Exam
A 65 year old male hypertensive, smoker presenting with sudden onset angina and managed as a case of ST elevation myocardial infarction in the anterolateral wall. At the emergency room his vital signs are as follows: BP 124/80mmHg, HR 95bpm, RR 20cpm. Pink palpebral conjunctiva, non-engorged neck veins, clear breath sounds, apex beat at 5th intercostal space midclavicular line with no murmur, good peripheral pulse.
Relevant Test Results Prior to Catheterization
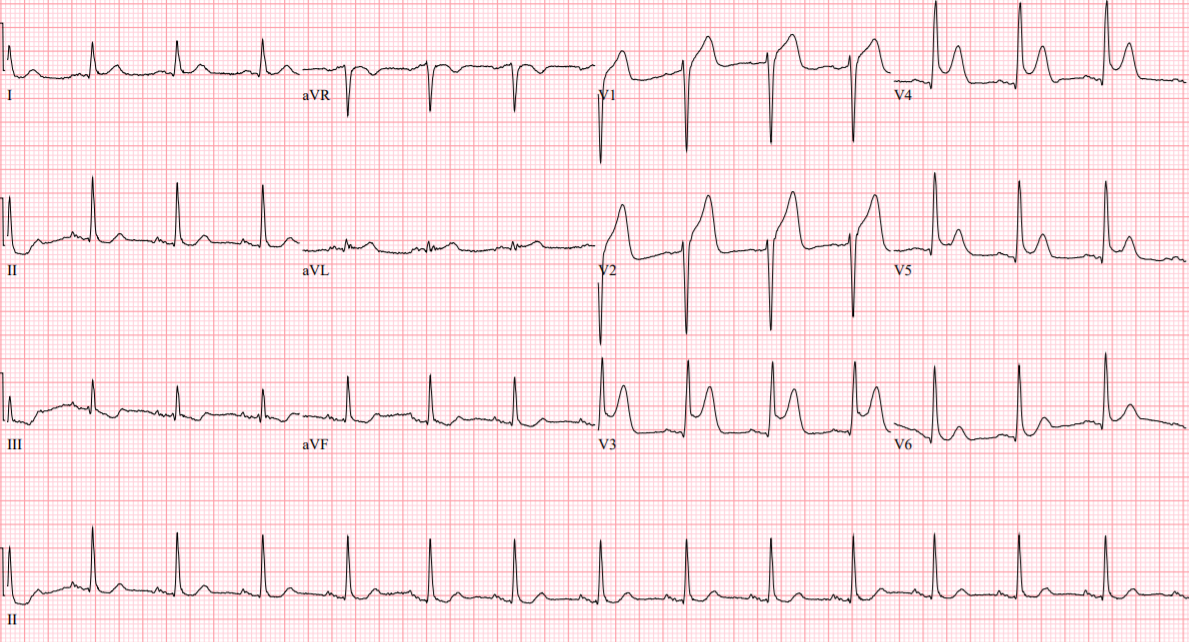
12 lead electrocardiogram showed normal sinus rhythm with ST elevation in leads V1-V5. Chest Xray showed atherosclerotic aorta with degenerative osseous changes.
Relevant Catheterization Findings
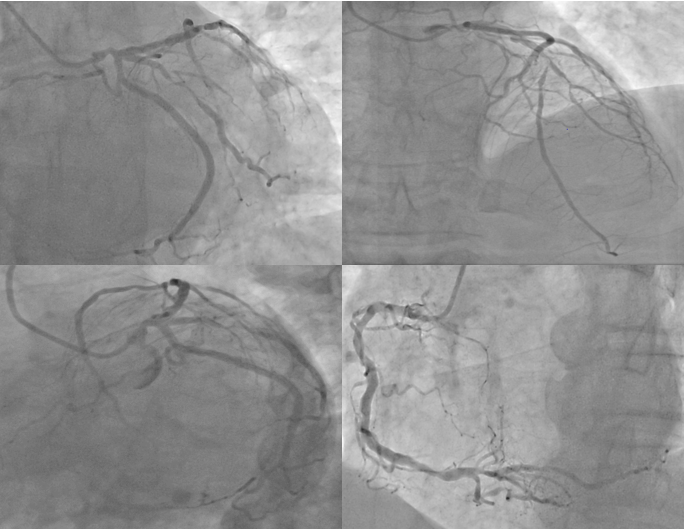
LMCA is a 4.2mm vessel with 60-70% distal segment stenosis. It trifurcates into LAD,ramus intermedius,and LCx.LAD is a 3.5mm diffusely diseased type III vessel with tandem stenosis of 60% at its proximal segment followed by a 90% mid segment stenosis. Ramus intermedius is a 3.5mm vessel with 80-90% proximal segment stenosis. LCx is a 3.5mm vessel with luminal irregularities at its proximal segment. RCA is a 3.5mm dominant vessel with 40% proximal segment stenosis and 50% distal segment stenosis.
 FV LAO CAUD.avi
FV LAO CAUD.avi
FV LAD CA.avi
Interventional Management
Procedural Step
1. Guide: 6F XB 3.5Coronary wire distalized to the LAD2. Predilation: 2.0x20mm balloon catheter positioned at mid LAD and inflated at 14ATM3. Stent: DES 2.5x30mm positioned at mid LAD lesion and deployed at 12ATMAnother coronary wire distalized to ramus intermedius(RI)4. Predilation: 2.0x20mm balloon catheter positioned at proximal RI lesion and inflated at 15ATM5. Stent: A second DES 2.5x30mm positioned at proximal RI lesion and deployed at 12ATM6. Stent: A third DES 3.5x9mm positioned at the LMCA and deployed at 12ATM7. POT: Using the same stent balloon at 15ATM8. Post deployment angiography: TIMI2 flow over the LAD with a consideration of plaque shiftMultiple wires used to attempt recrossing the stent struts to LAD but failed9. IVUS run of RI: Showed complete stent apposition of RI to LMCA stent with no carina shift to LAD10. Sasuke(Asahi,Japan) double lumen catheter positioned at the RI with side port facing the LAD allowed a Miracle 12 wire to cross the stent struts however failed to allow a 1.20x20mm balloon to cross11. Caravel microcatheter(Asahi,Japan), a 1.25x12mm balloon was able to cross the stent struts and inflated struts to the LAD at 16-20ATM, later upsized to a 2.0x20mm balloon inflated at 20ATM12. Stent: Using Culotte technique, a 3.0x32mm DES was positioned at the distal LMCA to the proximal LAD and inflated at 12ATM13. Postdilation: POT, FKBI, POT done using 4.0x9mm balloon14. Post PCI angiography: No residual stenosis, dissection, perforation with TIMI 3 flow
LAO CAUDAL post LMCA stent deployment showing TIMI 2 flow over the LAD.avi
Final Post PCI angiogram.avi
Case Summary
A complex PCI such as in this case can be safely done via transradial approach. However, coronary angiography alone cannot predict side branch compromise, and an IVUS guidance is essential for proper assessment of plaque morphology, lesion extent, and vessel diameter to avoid such complications. A bail out strategy using a Sasuke double lumen catheter provided adequate support and improved operability of our guidewire thus aided us in crossing the stent struts to the LAD. A Caravel microcatheter gave ample assistance as well for the balloon catheter to cross and open the stent struts to the LAD and proceed with the planned stenting technique.