
CASE20210810_004
Left Main Bifurcation Stenting Done by Different Techniques under IVUS & Physiology Guidance Advantages over One Another : A Case Series
By
Presenter
Rohit Mody
Authors
1
Affiliation
, India1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Left Main Bifurcation Stenting Done by Different Techniques under IVUS & Physiology Guidance Advantages over One Another : A Case Series
1
, India1
Clinical Information
Patient initials or Identifier Number
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
99200, 211649 & 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
Case 1- 99200 Case2- 211649 Case 3- 189914
99200, 211649 & 189914
Relevant Clinical History and Physical Exam
Case1-54 Year Old Male Post PTCA to LAD with Sirolimus Eluting DES 5 years back Hypertensive Diabetic Case2- 53-year-old Male Diabetic ACS- Ongoing Chest Pain with ECG changes Case 3- 80 years old Male AOE 3 DOE 3 Diabetic Hypertensive
Relevant Test Results Prior to Catheterization
Case 1-
Severe LV dysfunction
RWMA in LAD territory, EF-26%
Presented with Angina at rest, since 3 days diagnosed NSTEMI
Case 2-
ACS- Ongoing Chest Pain with ECG changes
Case 3-
Normal LV Function
Relevant Catheterization Findings
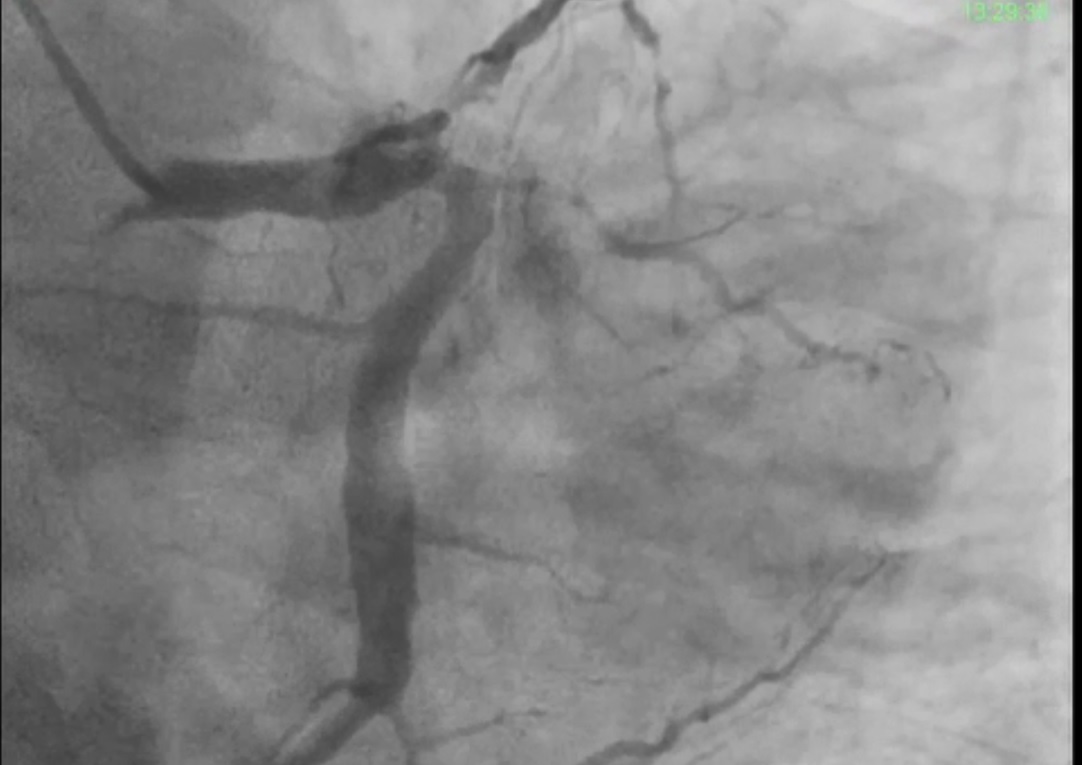
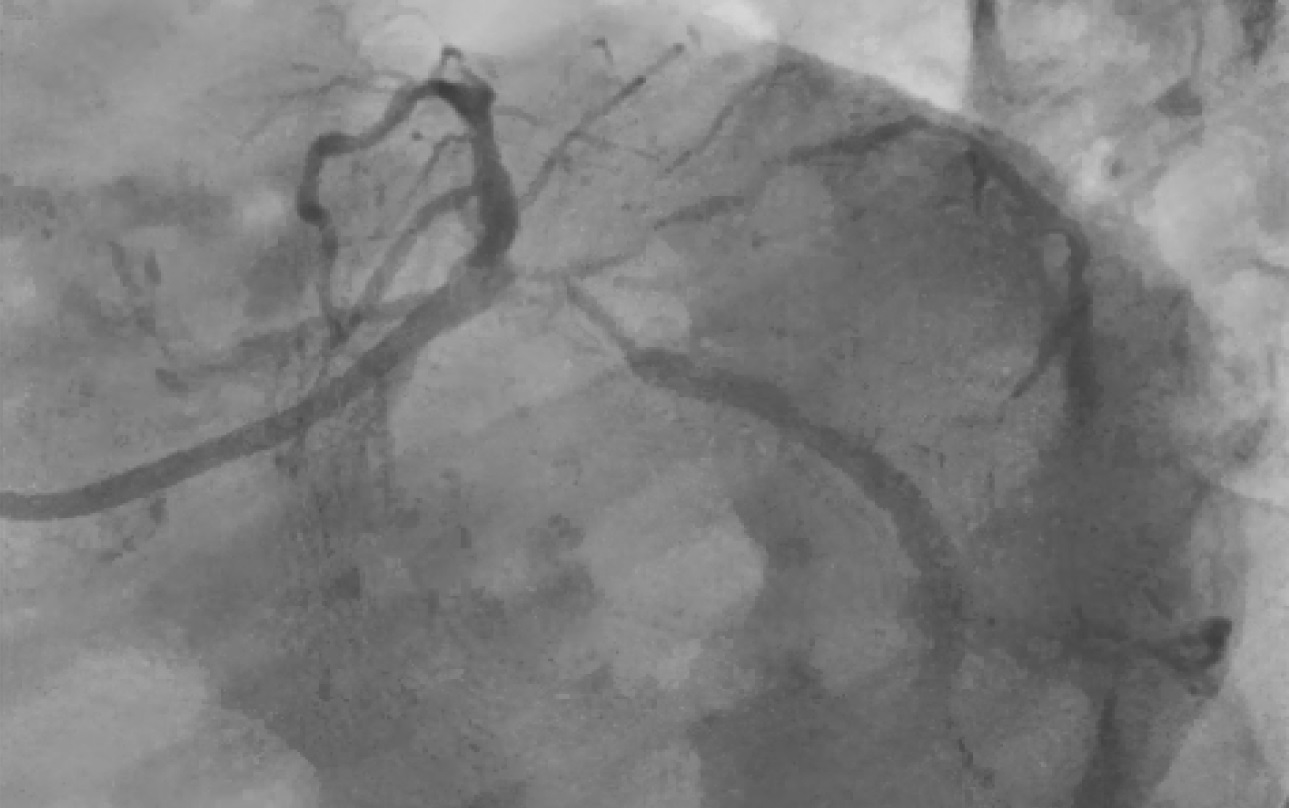
Case 1- NSTEMI came with ongoing chestpain CAG showed LM with TVD Case 2- Patient came with ACS, multiple risk factors, LM diseased, with very large left main, and relatively smalled LAD& LCX Medina 1:1:1. Case3- severe symptoms, CAG showed Medina 1:1:1.

Interventional Management
Procedural Step
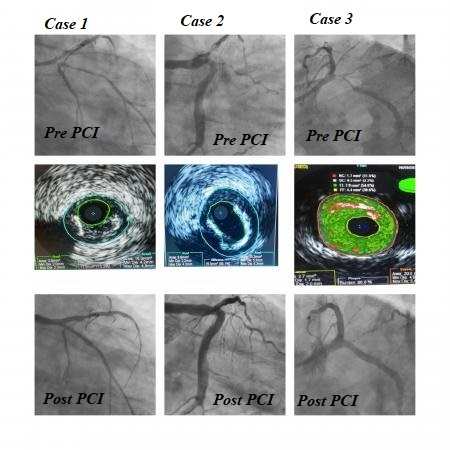
Case 1- Angiographic Results-Distal LM diseased with TVD, LAD proximal showing restenosis with clot,IVUS, BMW Wire crossed & 2.5x38mm Stent Deployed at 14ATM in distal LAD, 4x23mm Stent Deployed in LM to LAD at 16,POT done with 5.0x8mm balloon at 18ATM,2.5x33mm Stent to OM & KBT,POT done to LMCA. IVUS. Good final angiographic results.
Case 2- Angiography,Wire crossed &Predilated with 2.5x12mm balloon at 12 ATM,2.75x38mm in LM to LAD at 18ATM & 4.0x23mm in LM to LCX,KBT. final angiography shows good results.
Case3- Angiography,Rota LM to LCX with 1.5mm Burr,LAD crossed and Rota LM to LAD 1.5 mm Burr,LAD distal stent 3*38mm Post dilated at 18 ATM with 3.5*13 Balloon,LCX 4*38mm ostial Stent post dilated 4*10mm at 18 ATM,POT done to LCX stent,LAD stented from LM through Struts,LCX & LAD stent recrossed and Dilated,POT done, Final angiography shows good results.
Case Summary
Multilayered Provisional strategy remains treatment of choice for Left Main Bifurcation Lesions. In Provisional stenting Second stent can be deployed is and when required.There is a considerable role of IVUS Imaging and Physiology in optimizing the results and improving outcomesCulotte's technique can be used as a provisional stent strategy double kissing Culotte should be preferred technique.In Patients who present as ACS, SKS is still a viable technique. It is especially useful if Caliber of Left Main is too large and branches of LAD and LCX are disproportionately small.