
CASE20210812_002
Nonagenerian High Risk ACS with Rotablation LM PCI
By , ,
Presenter
Hashrul Rashid
Authors
1, 1, 1
Affiliation
, Australia1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Nonagenerian High Risk ACS with Rotablation LM PCI
1, 1, 1
, Australia1
Clinical Information
Patient initials or Identifier Number
JT
Relevant Clinical History and Physical Exam
90 year old lady presented to our hospital with a NSTEMI. She developed chest pain at home and later called the ambulance.
PMHx: Hypertension, hypercholesterolaemia, previous pacemaker (AV block).
Social Hx: Independent from home, non-smoker, mobilises with a 4-wheel frame.
Examination: BP 85-90/50. HR 90 bpm. Saturations 99% on 2L oxygen.
PMHx: Hypertension, hypercholesterolaemia, previous pacemaker (AV block).
Social Hx: Independent from home, non-smoker, mobilises with a 4-wheel frame.
Examination: BP 85-90/50. HR 90 bpm. Saturations 99% on 2L oxygen.
Relevant Test Results Prior to Catheterization
ECG: RBBB
Troponin: 27,000 ng/L
Hb 125 g/L
Creatinine 110 micromol/L
Troponin: 27,000 ng/L
Hb 125 g/L
Creatinine 110 micromol/L
Relevant Catheterization Findings
LM: Critical (99%) calcified distal stenosis before trifurcating into three large calibre arteries (Medina 1,1,1,0).
LAD: The ostial LAD had critical (99%) stenosis. There were minor irregularities throughout the remaining segments.
Ramus: Minor irregularities.
LCx: Severe (80%) stenosis in the ostial LCx. There were minor irregularities throughout the remaining segments.
RCA: Dominant vessel with minor irregularities.
Ventriculogram: Severe LV dysfunction with anterior hypokinesis.
RCA: Dominant vessel with minor irregularities.
Ventriculogram: Severe LV dysfunction with anterior hypokinesis.
Interventional Management
Procedural Step
Pre-PCI planning:
- Left femoral artery - delivery of intra-aortic balloon pump, at 2:1 setting.
- Right femoral artery - 7F EBU 3.5 guide.- PCI plan was to image with OC, rot ablation then provisional PCI of LMCA to LAD.
1) Rotablation and OCT:
- Fielder XTR delivered to distal LAD then exchange with rotawire using micro catheter.
- 4 runs of 1.5 mm rotaburr at 160,000 rpm (Video 1)
- Sion Blue wires to LAD and LCx
- 2.5mm non-compliant (NC) balloon to LMCA-LAD and LCx
- OCT revealed some plaque modification of LAD and LCx, which were heavily calcified.
2) Provisional PCI LMCA-LAD
- Still planning provisional LMCA-LAD.
- 3.0 mm NC balloon to LMCA-LAD
- 3.5 x 23mm Xience from LMCA-LAD (stent sizing from OCT) (Video 2).
- Stent post-dilated with 4 x 12mm and 5 x 8 mm NC balloons to LAD and LMCA, respectively.
- Kissing Balloon Inflation (KBI) with LMCA-LAD/LCx using 4 x 12 and 3x15 NC balloons to LAD and LCx respectively.
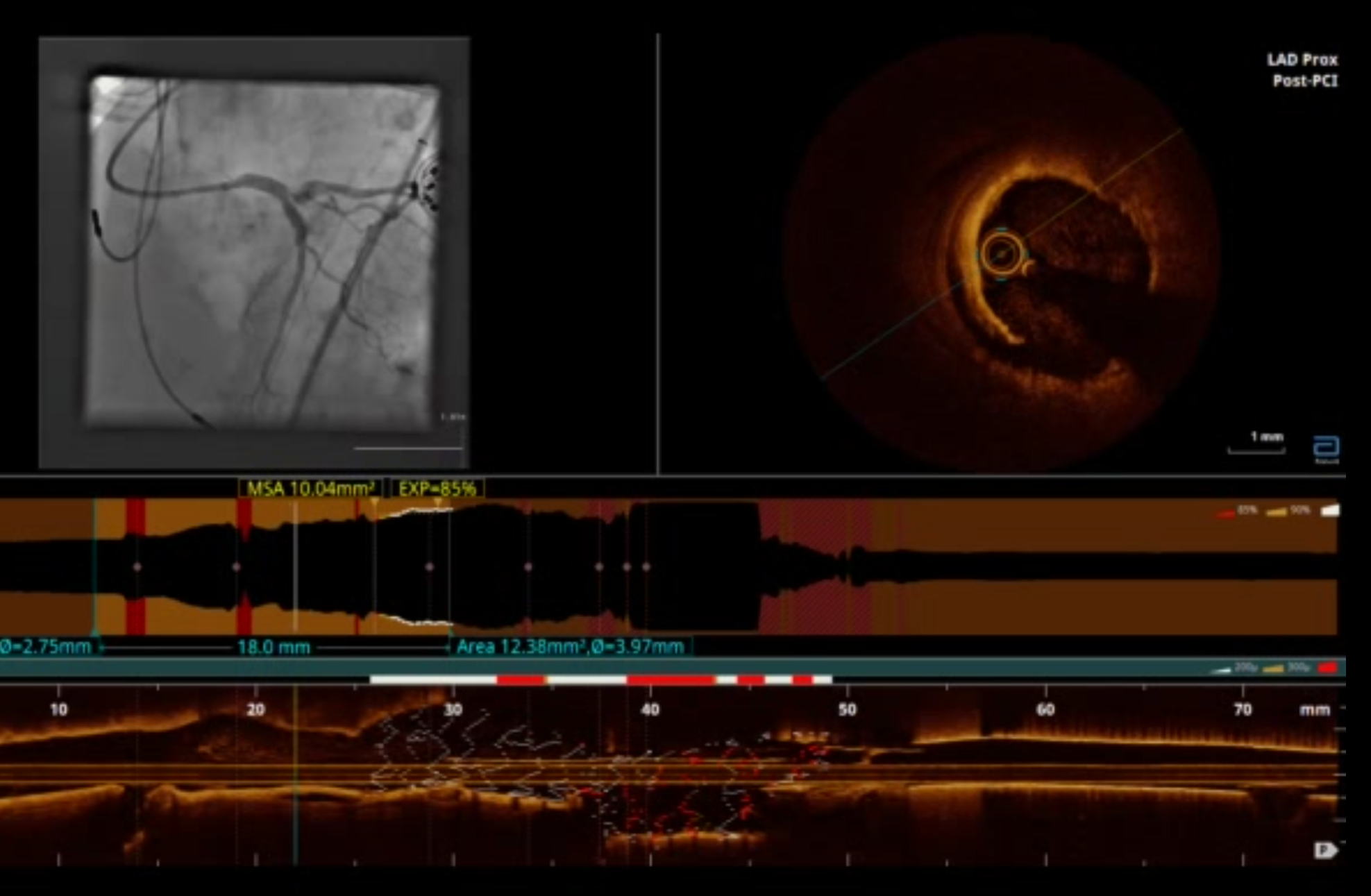
3) OCT and further PCI
- OCT revealed distal edge dissection to LAD stent (Image 1), so further PCI with 2.5.x18 mm Xience then post-dilated with 3x18mm NC balloon.
- Angiographically, ostial LCx was severe (90%) stenosed (Video 3), so pre-dilated with 3x15mm NC balloon.
- With TAP procedure, a 3.5x12mm Xience delivered to ostial LCx then KBI with stent balloon (LCx) and 4x15mm NC (LAD)
- Edge dissection of LCx stent (Video 4), so a 2.5x18mm Xience stent delivered to proximal LCx, then post-dilated up to 3.0mm NC balloon.
Angiographically good result (video 5).
Case Summary
Mrs. JT was a 90yo lady who presented in cariogenic shock with high risk NSTEMI and calcified distal LMCA stenosis trifurcation. She had intra-aortic balloon pump for haemo-dynamic support and rotablation to the LMCA.
We PCI the LMCA-LAD (provisional) with a 3.5 x 23 mm Xience then post-dilate with 4.0mm and 5.0 mm NC balloons. There was a distal edge dissection on OCT, so a 2.5 x 18 mm Xience was delivered to the proximal-mid LAD.
Due to residual ostial LCx disease, a 3.5 x 12 mm Xience delivered for TAP stenting procedure with KBI. Residual distal edge dissection treated with a 2.5 x 18mm Xience stent toproximal-mid LCx. Angiographically good outcome. Patient discharged day 5 with no issues.
We PCI the LMCA-LAD (provisional) with a 3.5 x 23 mm Xience then post-dilate with 4.0mm and 5.0 mm NC balloons. There was a distal edge dissection on OCT, so a 2.5 x 18 mm Xience was delivered to the proximal-mid LAD.
Due to residual ostial LCx disease, a 3.5 x 12 mm Xience delivered for TAP stenting procedure with KBI. Residual distal edge dissection treated with a 2.5 x 18mm Xience stent toproximal-mid LCx. Angiographically good outcome. Patient discharged day 5 with no issues.