
CASE20210815_001
Perforation a Cathlab Nightmare How to Get Out of This Critical Complication
By
Presenter
Rohit Mody
Authors
1
Affiliation
, India1
Complications - Complications
Perforation a Cathlab Nightmare How to Get Out of This Critical Complication
1
, India1
Clinical Information
Patient initials or Identifier Number
Case 1- 142741 Case 2- 168707 Case 3- 193675 Case 4- 202678
Case 1- 142741 Case 2- 168707 Case 3- 193675 Case 4- 202678
Case 1- 142741 Case 2- 168707 Case 3- 193675 Case 4- 202678
Relevant Clinical History and Physical Exam
Case1- Female 43 year old, Non Q- Anterior MI, Diabetic Case2- Female 67 year old, Acute Anterior MI, ischemic time 72 hrs. post MI angina, Diabetic Case3- Male 46 year old, Acute Breathlessness, LVF, Severe LV dysfunction on ECHO, EF 20%,Troponin Raise hence, diagnosed ACS Case4- 77 Year old female, Hypertension, Diabetes Mellitus-2
Relevant Test Results Prior to Catheterization
Case 1- Normal LV FunctionCase 2- EF 40%, LV DysfunctionCase 3- EF 30%, RWMICase 4- Normal LV function
Relevant Catheterization Findings
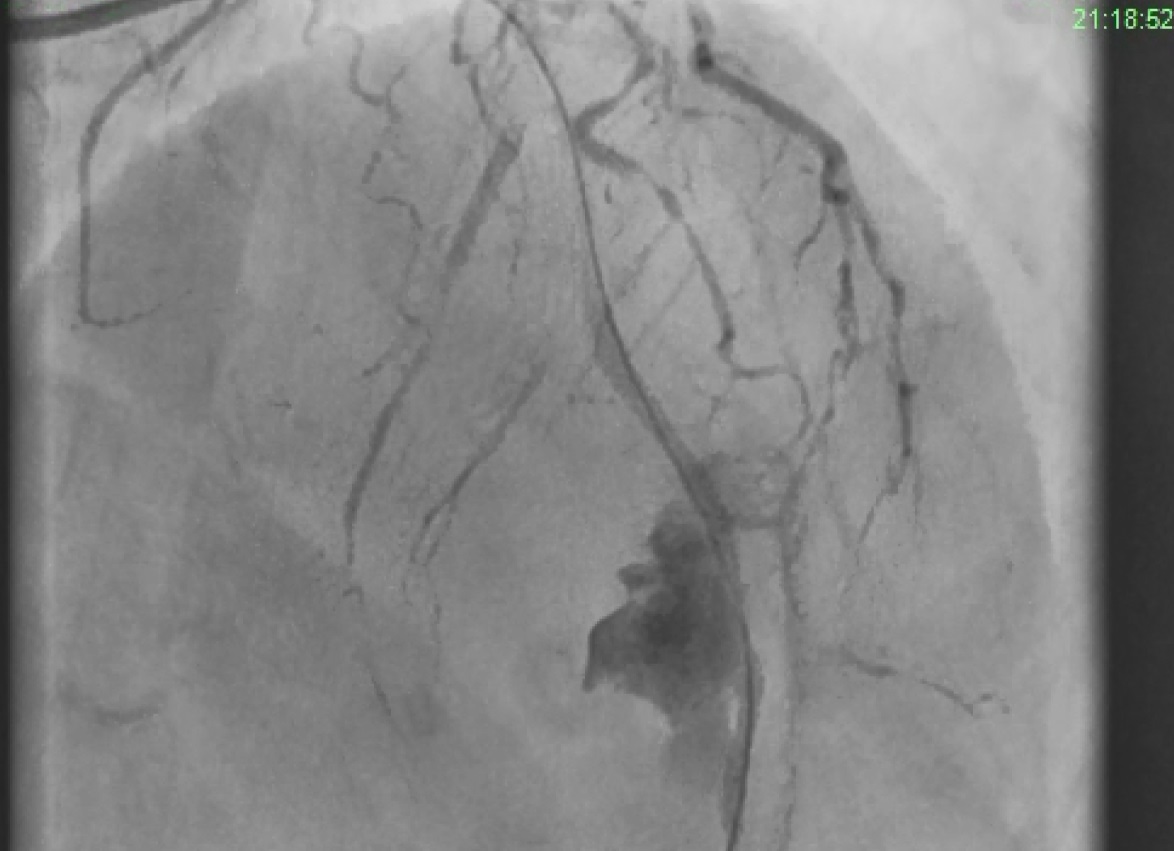
Case1- SVD, mid LAD 98%
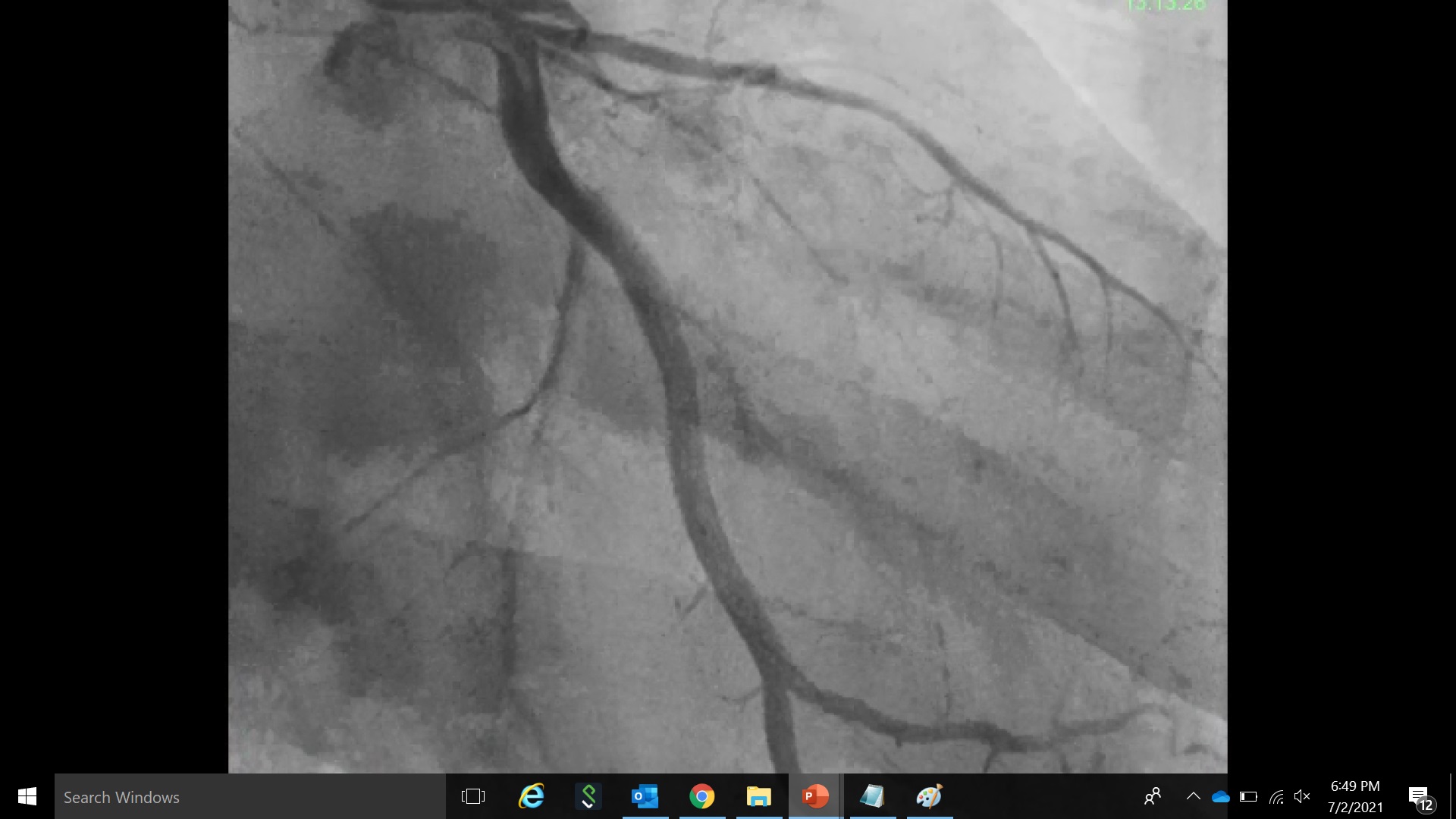
Case2- DVD, Planned to do culprit vessel PTCA, stent to LAD
Case3- LAD 100% & RCA normal
Case4- Angiography revealed LAD 90%

Case2- DVD, Planned to do culprit vessel PTCA, stent to LAD
Case3- LAD 100% & RCA normal
Case4- Angiography revealed LAD 90%
Interventional Management
Procedural Step
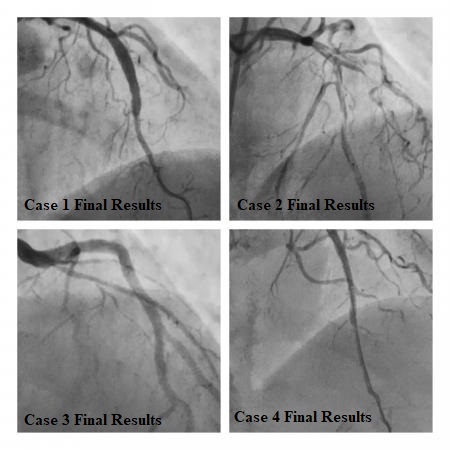
Case1- Crossed with wire Balloon dilated, stent deployed 3.0X34mm at 18 ATM, Type 3 Perforation occurred at Middle of the stent. Peri- cardio centesis done immidiatelyPerforation was sealed with stent graft 3.5X20 mm Graftmaster.
Case2- Lesion crossed with wire, sequentially balloon dilatated with balloon, Then stent deployed 2.5X48mm, vessel was calcified and small diameter. Post dilation done which lead to Type 3 perforationPeri- cardio centesis done immediately, Cover stent graftmaster2.8X19 deployed, Perforation sealed with broken balloon and stent graft at the perforation site.
Case3- Distal LAD was not at all visible, With difficulty and manipulation crossed with wire Fielder FC coated wire, Then predilated with a 1.25mm balloon, Type 3 Perforation occurred at Distal LADImmediately in proximal LAD balloon was dilated & perforation sealed temporarily. Finally, the bleeding stopped patient clinically stable.
Case4- BMW coronary guidewire crossed with Balloon support,2.5X44mm DES Deployed distally at 16 atm.3.5x24mm DES deployed at 18 atm. Check angio was done which shows Type 3 Perforation, Graftmaster (covered stent) 2.80x26mm deployed at 16 atm.
Case Summary
1. Type 3 perforation is dreaded complication urgent peri-cardio centesis and sealing is important.2. Sometimes the complications help in bailout.3. Calcific nodules pose significant risk.4. Modification Pre-stenting is essential.