
CASE20210817_001
Rotablation and Kissing Drug-Coated Balloons for a Critical In-Stent Restenosis in Left Main Bifurcation in a Patient with Angina CCS Class IV and a Low Left Ventricular Ejection Fraction
By ,
Presenter
Udin Bahrudin
Authors
1, 1
Affiliation
, Indonesia1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Rotablation and Kissing Drug-Coated Balloons for a Critical In-Stent Restenosis in Left Main Bifurcation in a Patient with Angina CCS Class IV and a Low Left Ventricular Ejection Fraction
1, 1
, Indonesia1
Clinical Information
Patient initials or Identifier Number
SWP
Relevant Clinical History and Physical Exam
A 53-year-old man with recurrent chest pain at rest (CCS class IV) was referred to our cath. lab. for urgent PCI, with coronary risk factors: hypertension, uncontrol DM and CKD on hemodialysis. Physical exam was unremarkable.
Relevant Test Results Prior to Catheterization
ECG and echocardiogram showed anterior wall ischemia and hypokinesis, respectively, with LVEF 39%. Six months prior to the presentation, a PCI of calcified LM-LAD-LCx with rotablation was done and 4 DES were implanted.
Relevant Catheterization Findings
Coronary angiography revealed a critical in-stent restenosis (ISR) in distal LM bifurcation with 1,1,1 Medina classification, while a borderline stenosis in distal RCA.
Interventional Management
Procedural Step
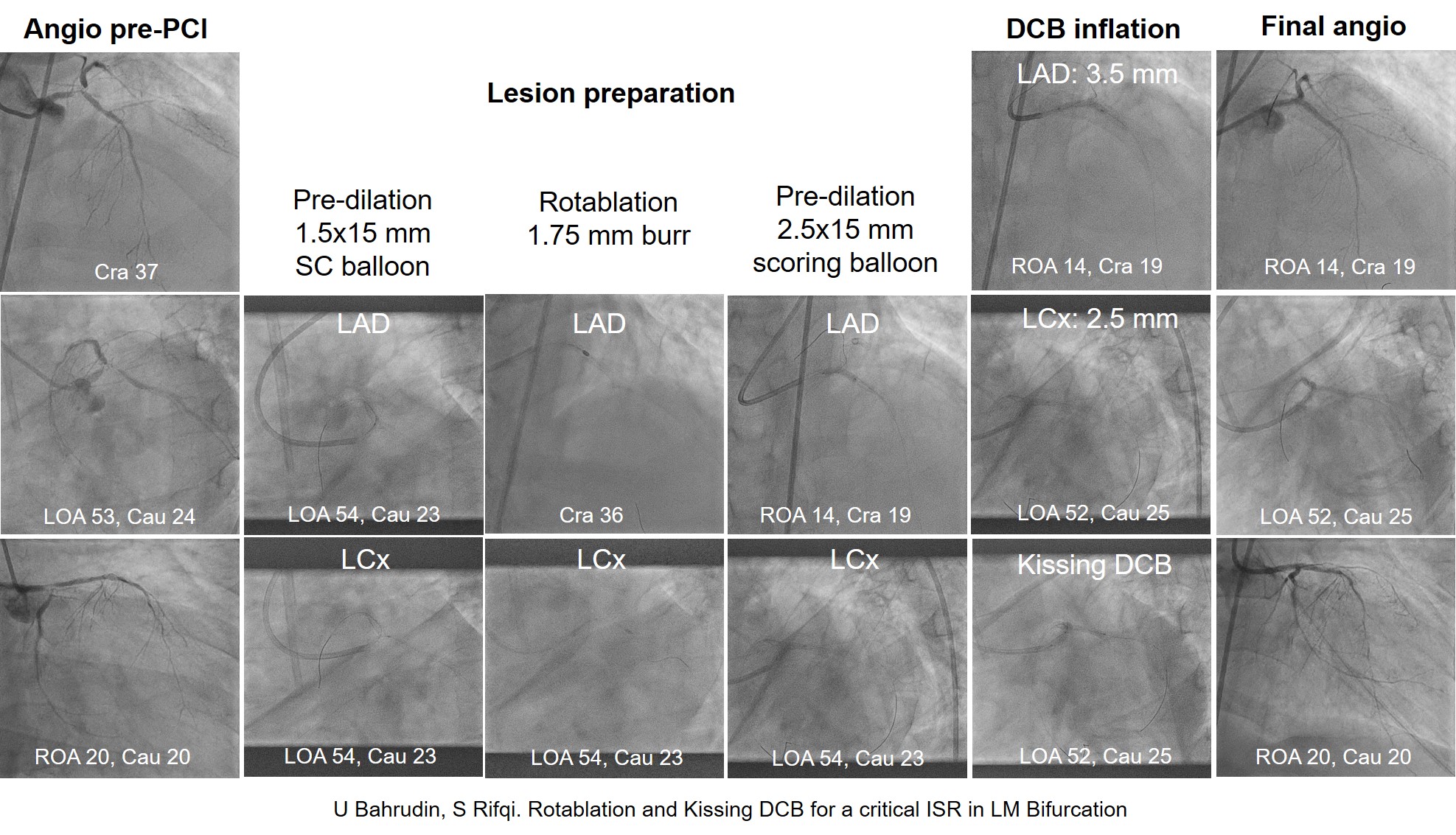
He was proceeded to PCI at the LM bifurcation. A floppy wire was inserted to LM-LAD while a 1.5x15 mm semi compliant (SC) balloon has been placing on the wire. The balloon was then quickly moved to the LM-LAD critical stenosis and then inflated. Another floppy wire was inserted to LM-LCx and the SC balloon was then inflated. RA (Rotablator, Boston) was then performed with a 1.75 mm burr gradually advanced at 150,000 rpm to passed the subsequent lesions of LM-LAD and LM-LCx. Furthermore, a 2.5x15 mm scoring balloon was used to prepare the lesions. Drug-coated balloons (DCB), 3.5x20 mm and 2.5x20 mm, were deployed at the LM-LAD and LM-LCx, subsequently, and followed by a kissing balloon inflation using those balloons in the bifurcation. Final angiogram showed no residual stenosis and TIMI 3 flow. During the procedures, the patient was experienced an acute lung edema and relieved by medications. He had no any symptom at 12 months follow up post PCI.
Case Summary
PCI of a critical ISR in LM bifurcation in a patient with angina CCS class IV and a low LVEF was successfully done with a quick balloon dilatation followed by rotablation and finalized with kissing DCB inflation.