
CASE20210819_001
Efficacy of King Ghidorah Technique Prior to Simultaneous V-stenting for Thrombotic Occluded Left Main Coronary Artery: A Case Report
By , , , , , , , , , , , , ,
Presenter
Tatsuhiko Ito
Authors
1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 1
Affiliation
, Japan1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Efficacy of King Ghidorah Technique Prior to Simultaneous V-stenting for Thrombotic Occluded Left Main Coronary Artery: A Case Report
1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 1
, Japan1
Clinical Information
Patient initials or Identifier Number
QQ
Relevant Clinical History and Physical Exam
A 55-year-old male suddenly collapsed and bystander cardiopulmonary resuscitation (CPR) was performed. Paramedics contacted after 6 minutes from the emergency request, and the first electrocardiogram showed ventricular fibrillation (VF). Although defibrillation with automated external defibrillation was conducted for 4 times, it failed to recover the spontaneous circulation (ROSC). At arrival, and percutaneous cardiopulmonary support (PCPS) was inserted, obtaining a spontaneous circulation.
Relevant Test Results Prior to Catheterization
Data at emergent room: pH 7.27, pCO2 53.6, pO2 256, HCO3 23.8, WBC 11.8 109/L, Hct 39.3 %, Cre 1.27 mg/dl, CK 212 U/L, CRP 1.46 mg/dl. He had the coronary risk factors of diabetes (HbA1c 6.6), hypertension, and current smoking. The electrocardiogram showed sinus tachycardia with ST-segment elevation in aVR and precordial leads from V1 toV4 leads. Emergent coronary angiogram(CAG) for anterior ST-segment elevated myocardial infarction (STEMI) complicated with cardiogenic shock was conducted.

Relevant Catheterization Findings
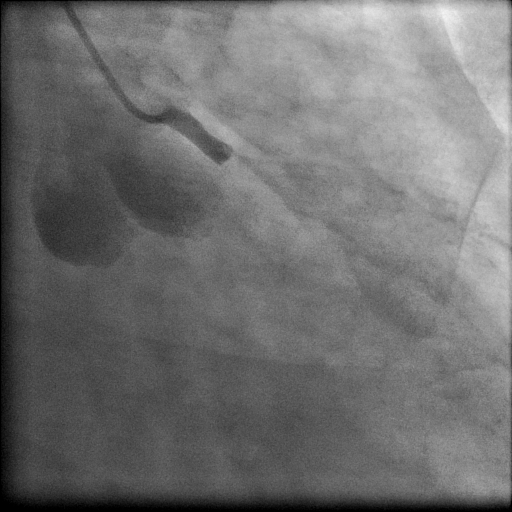
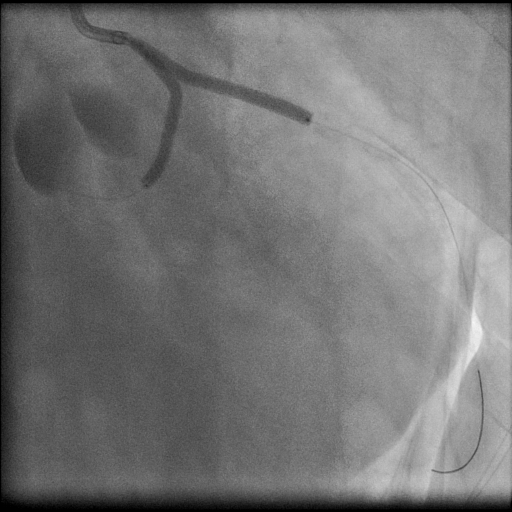
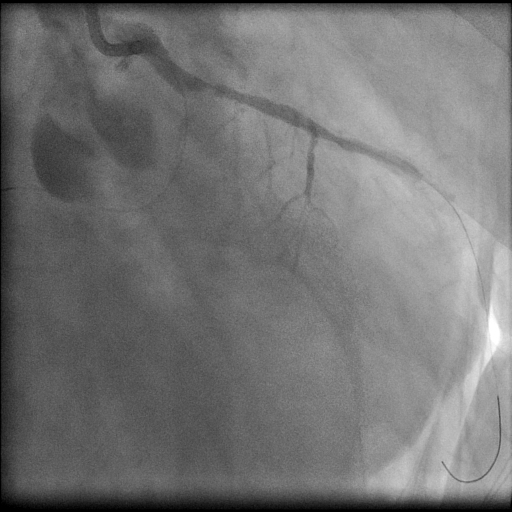
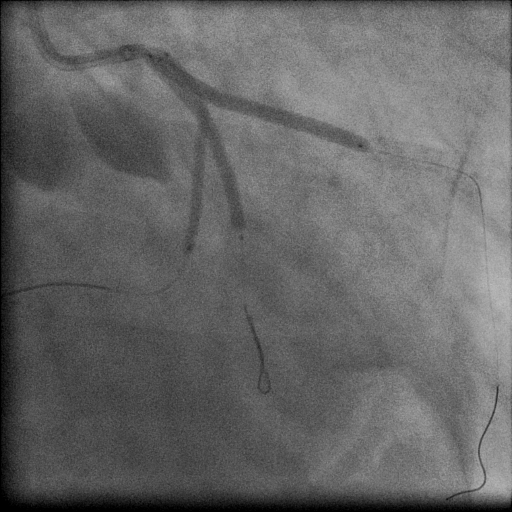
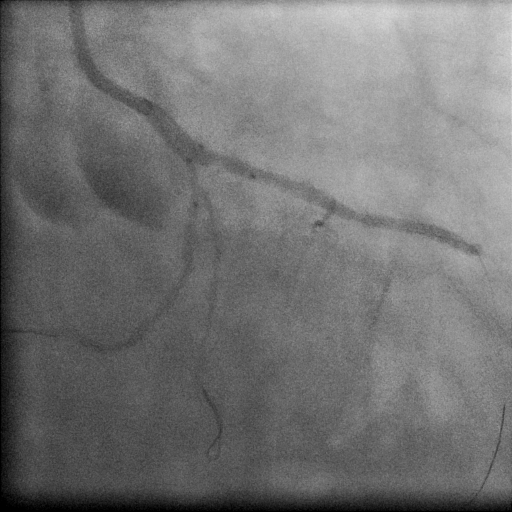
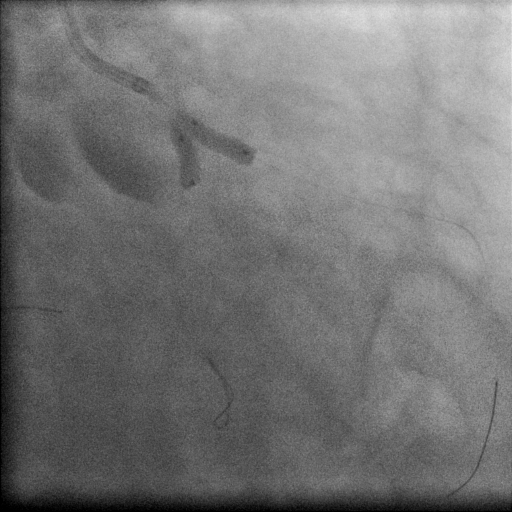
First angiogram showed the thrombotic occlusion of left main coronary artery (LMCA) (Figure 1). 8Fr extra-backup (EBU Launcher 3.5with side hole) was used. All of the pre-dilations using 2x40mm (Ryurei) of LAD, kissing ballooning technique (KBT) using 2.5x40 mm (LAD)and 2x40 mm (LCX),and 3 mm in LAD with 2.5 mm in LCX (Figure 2) failed to restore both of the flows of LAD and LCX with abrupt closures (Figure 3).
Interventional Management
Procedural Step
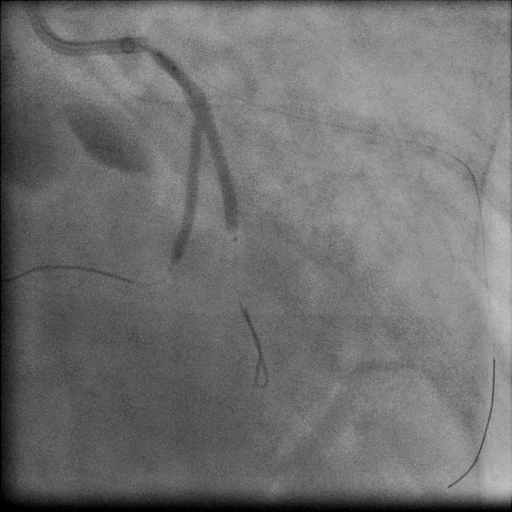
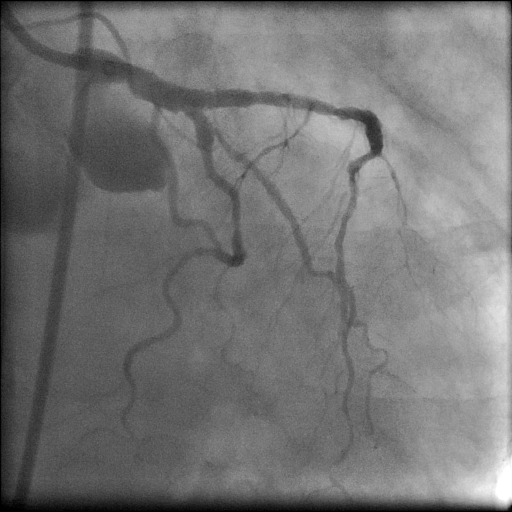
KBT to intra-LCX bifurcation (main vessel and obtuse marginal branch (OM)) also failed to increase the TIMI-grade flow of LCX (Figure 4). Therefore, the king ghidorah technique (KGT) using 3long (40mm) Ryurei balloons (LAD; 3mm, LCX 2 mm, and OM 2.5 mm) was conducted for thrombotic LMCA distal trifurcation (Figure 5). The inflation device for KGT was constructed by combining the inflation devices used for KBT (Figure 6).
Case Summary
The King ghidorah technique using long balloons for thrombotic occluded left main coronary artery using 8Fr guiding catheter was effective to simultaneously restore the flows of LAD and LCX, and to the subsequent stenting.