
CASE20210819_009
PCI and Stenting in a Long Segment CTO (ISR) in a Dominant RCA, Using the Antegrade Technique
By ,
Presenter
Harinder K. Bali
Authors
1, 1
Affiliation
, India1
Complex PCI - Chronic Total Occlusion
PCI and Stenting in a Long Segment CTO (ISR) in a Dominant RCA, Using the Antegrade Technique
1, 1
, India1
Clinical Information
Patient initials or Identifier Number
MSJ
Relevant Clinical History and Physical Exam
61 years old male, presented with complaints of exertional dyspnoea and angina. Patient was a known case of CAD, with history of inferior wall MI in 1996. He underwent PTCA to RCA with BMS at that time. This was followed by PTCA and stent to RCA in 1999, 2000 with BMS, PTCA and stent to RCA with DES in 2010, DEB to RCA in 2013.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
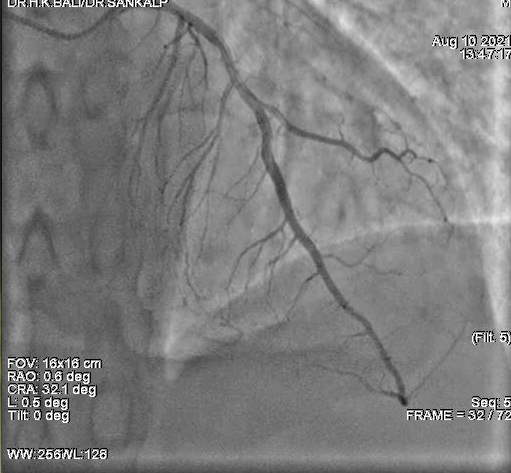
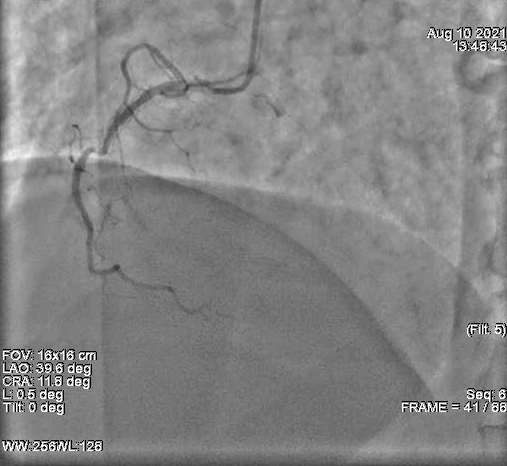
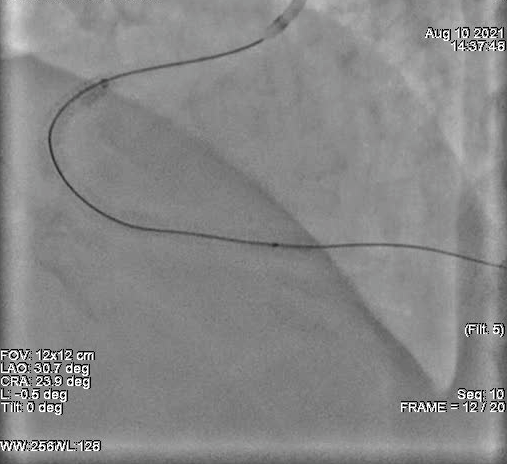
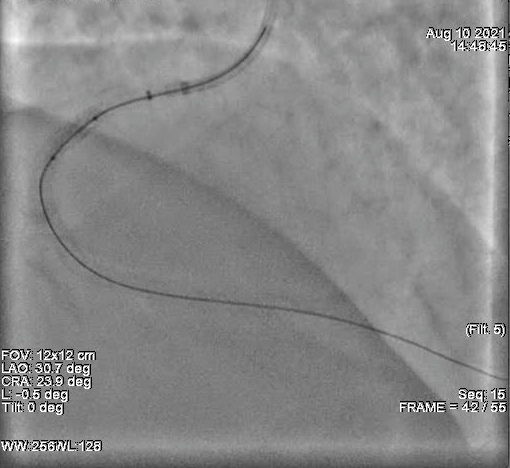
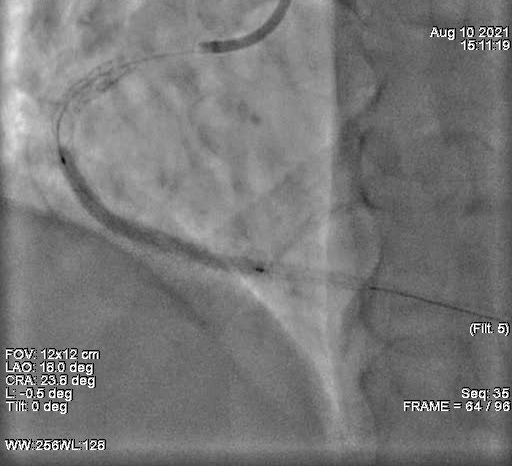
Patient underwent CAG for his symptoms, which revealed a dominant RCA with mid segment CTO with 100% ISR., with retrograde filling of the PDA and PLV. PTCA and stenting to RCA was planned.

Interventional Management
Procedural Step
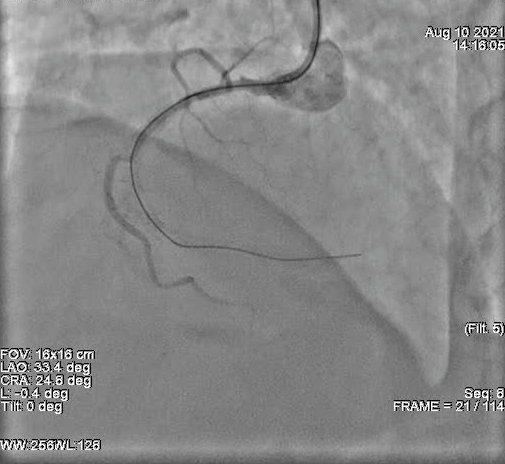
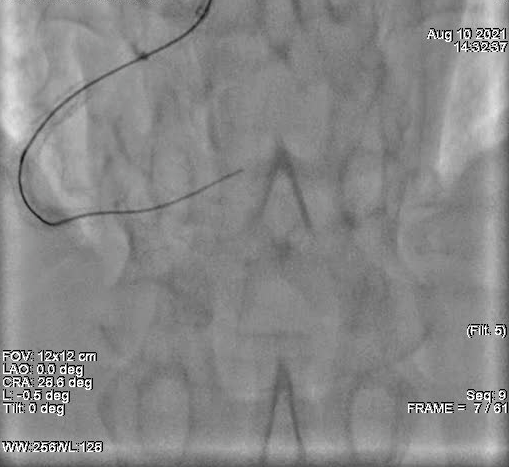
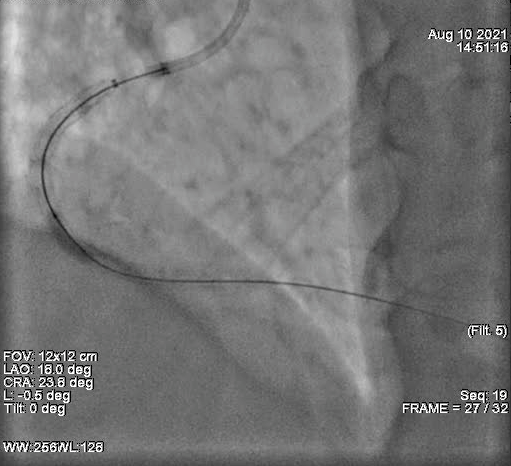
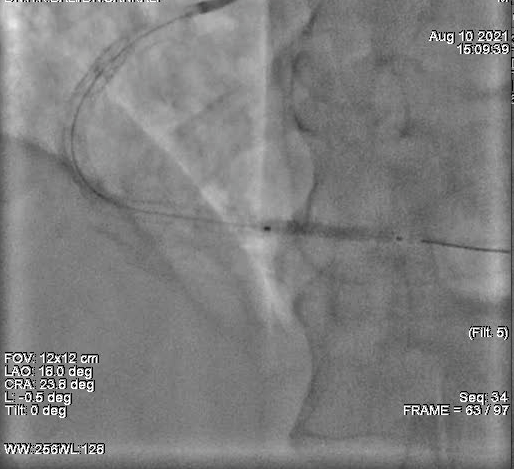
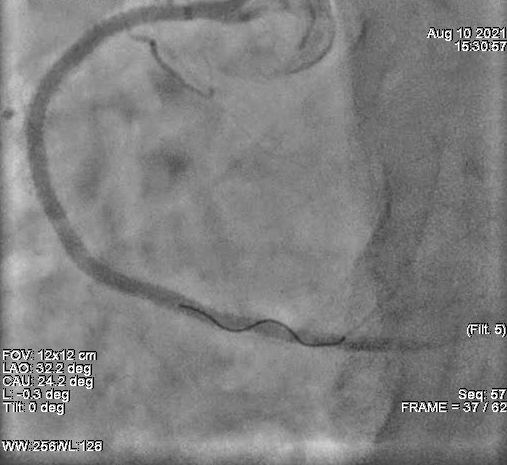
Successful PTCA and stenting for chronic total occlusion in dominant RCA ISR done using the antegrade technique. Route: right radial arteryGuiding catheter: 6f SCR 3.5Guidewires: Gaia second, Fielder XT, BMWAdditional hardware used: Telescope 6F, Asahi Caravel (micro catheter)Pre stent dilatation done with 1.25x10mm, 1.5x12mm, 2.0x12mm, 2.5x15mmXIENCE XPEDITION stents 3.0x48mm, 3.ox48mm and 2.5x23mm deployed in proximal RCA to Post stent dilatation done with 2.5x15mm, 3.0x12mm, 3.0x15mm NC balloons



Case Summary
Antegrade technique is useful for short segment CTO’s. However we successfully performed PCI and stenting in a long segment CTO where retrograde wiring was not possible, using the antegrade wiring technique.