
CASE20210819_010
Percutaneous Intervention in a Complex Left Main Trifurcation Lesion
By ,
Presenter
Harinder K. Bali
Authors
1, 1
Affiliation
, India1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Percutaneous Intervention in a Complex Left Main Trifurcation Lesion
1, 1
, India1
Clinical Information
Patient initials or Identifier Number
RR
Relevant Clinical History and Physical Exam
A 76 years old female, presented with complaints of chest pain and dyspnoea on exertion since the past one month, increased since last 2-3 days K/C/O DM 2. ECG revealed T wave inversions from V1 to V6 2D echo revealed RWMA with moderate MR, LVEF 50%
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
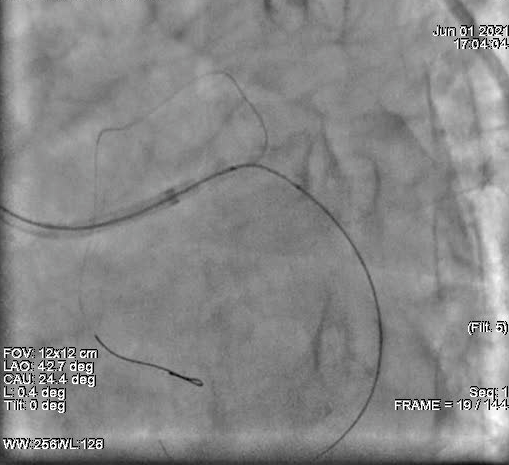
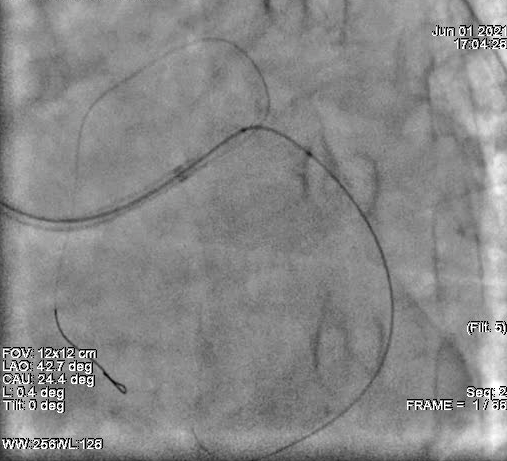
Procedure: Selective Coronary Angiography Route: Right Femoral Anesthesia: Xylocaine Hardware:6F JR 3.5, 6F JL 4.0 Contrast: Ornnipaque CORONARY PROFILE LM: Distal segment calcification noted involving ostillm of LCx LAD:Type III vessel. ostial 70-80% stenosis, mid and distal segment are normal. Diagonal: Normal Ramus: Normal LCx: Dominant, ostial calcific lesion with 99% stenosis. OM: Normal RCA: Non Dominant, Normal PDA: Normal PLV: Normal



Interventional Management
Procedural Step
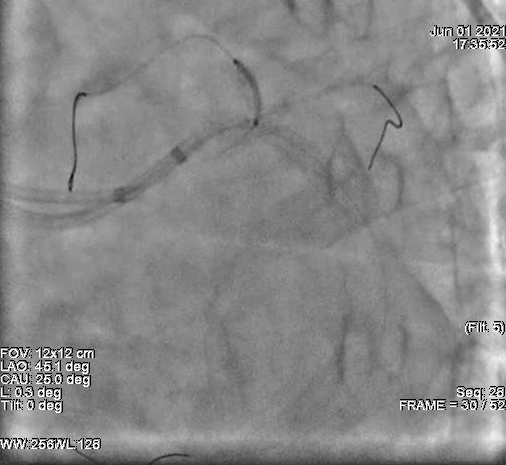
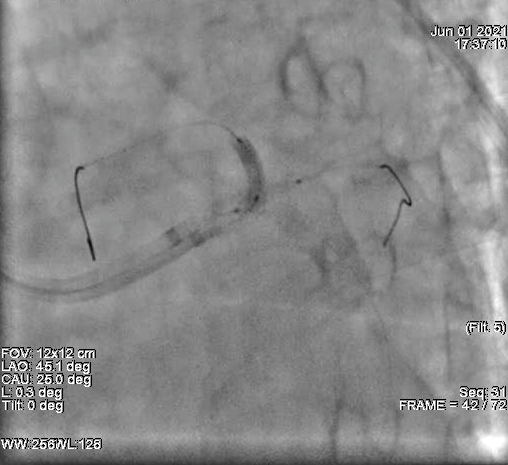
Procedure:PCI Left Main Trifurcation (TAP Technique) Route: Right/Left Femoral Artery Contrast:Omnipaque Anesthesia:2% Xylocaine (Local Anesthesia) Guiding Catheter: 7F EBU 3.5,6F EBU 3.5 Guiding Wire: Fielder XT,BMW(3) Balloon:Pre stent dilatation done with 2.0x15mm,2.5x15mm,3.0x15mm balloons Stent:RESOLUTE ONYX stent 4.0x30mm deployed in LM to LCx; XIENCE XPEDITION stent 2.75x23mm deployed in proximal LAD Balloon: Post stent dilatation done with 2.5x12mm,2.75x15mm,3.0x12mm,4.0x15mm,5.0x8mm NC balloons , Kissing Balloon dilation of trifurcation done with 2.75x15mm (LAD),2.5x12mm (Ramus),3.0x12mm (LCx) ,POT done with 5.0x8mm (LM) Additional Drug:Heparin 7500 units





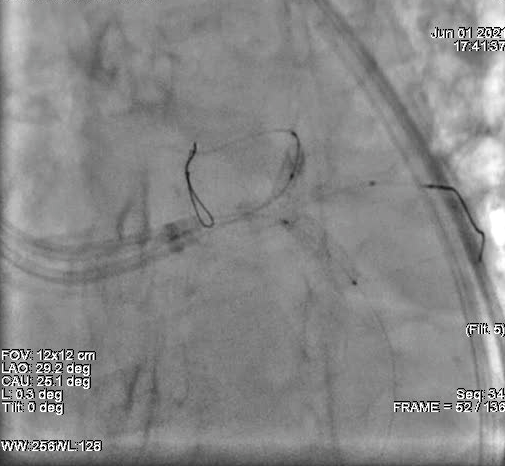
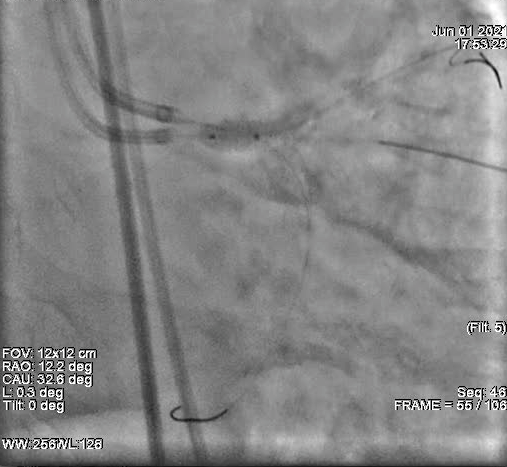
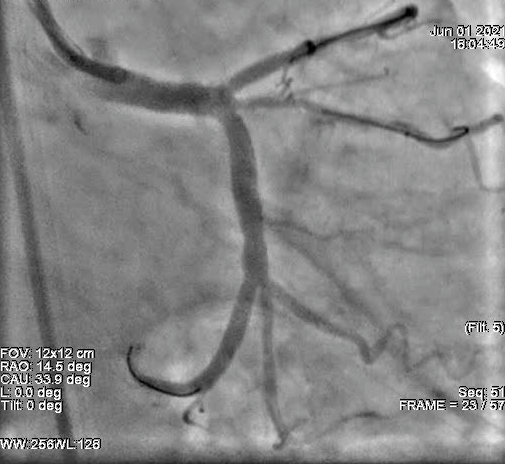
Case Summary
Successful percutaneous intervention done in a complex left main trifurcation leson, with stenting to LM-->LCx and LAD, and POBA to ramus.Procedure was uneventful and patient remained stable on follow up.