
CASE20210819_012
Intravascular Lithotripsy for Management of an Underdeployed Stent in Anomalous RCA and LAD ISR in the Same Sitting
By ,
Presenter
Harinder K. Bali
Authors
1, 1
Affiliation
, India1
Complex PCI - Calcified Lesion
Intravascular Lithotripsy for Management of an Underdeployed Stent in Anomalous RCA and LAD ISR in the Same Sitting
1, 1
, India1
Clinical Information
Patient initials or Identifier Number
RMS
Relevant Clinical History and Physical Exam
73 years old male, presented with angina, known case of coronary artery disease, had previously undergone PTCA and stenting to LAD in 2017
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
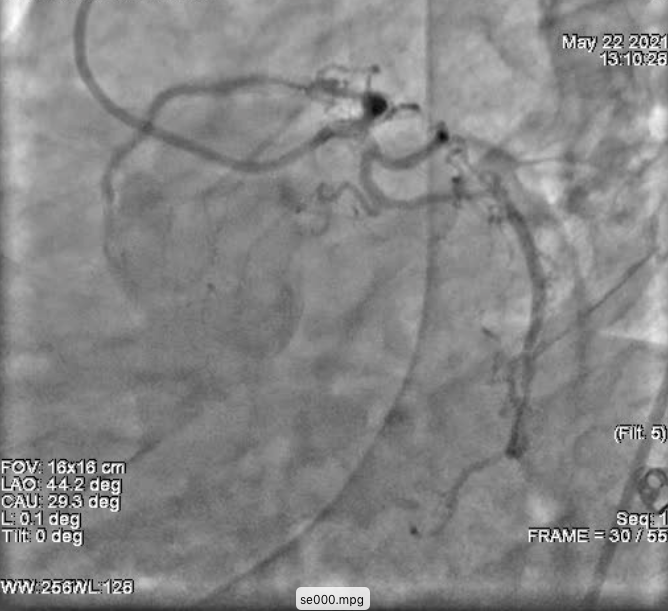
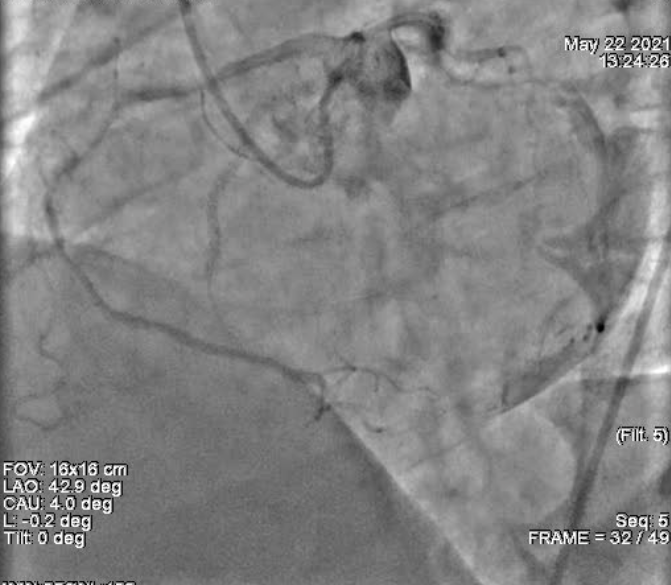
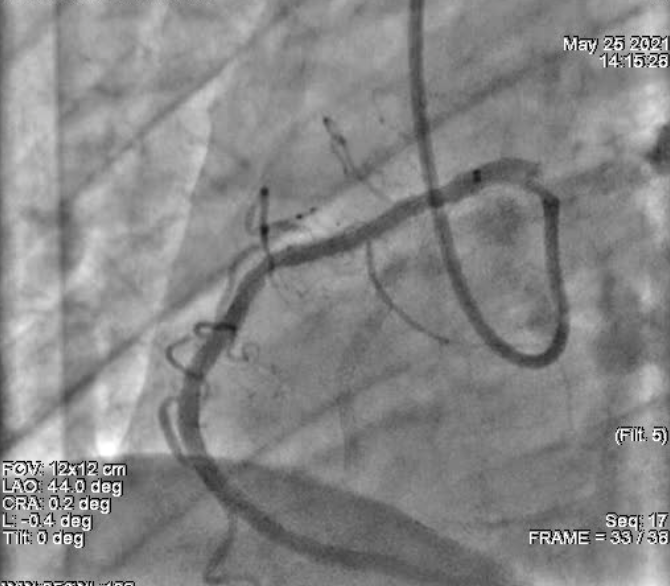
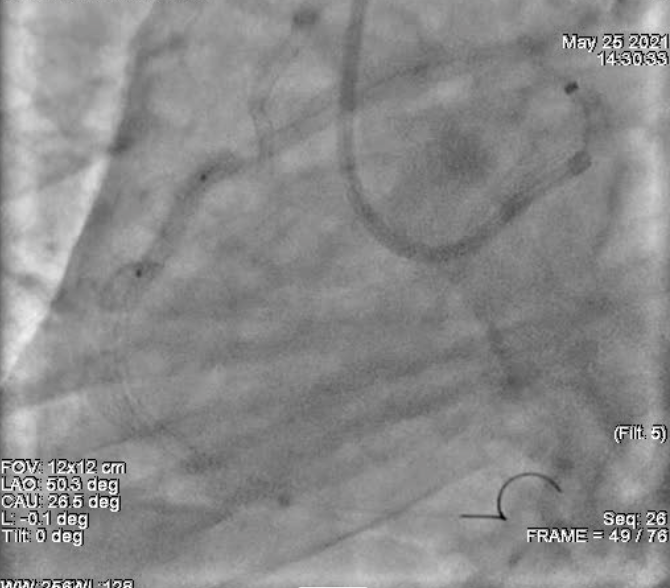
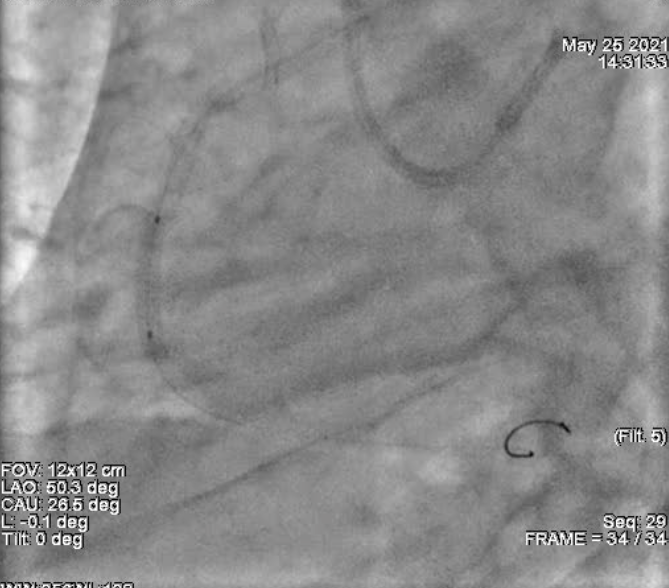
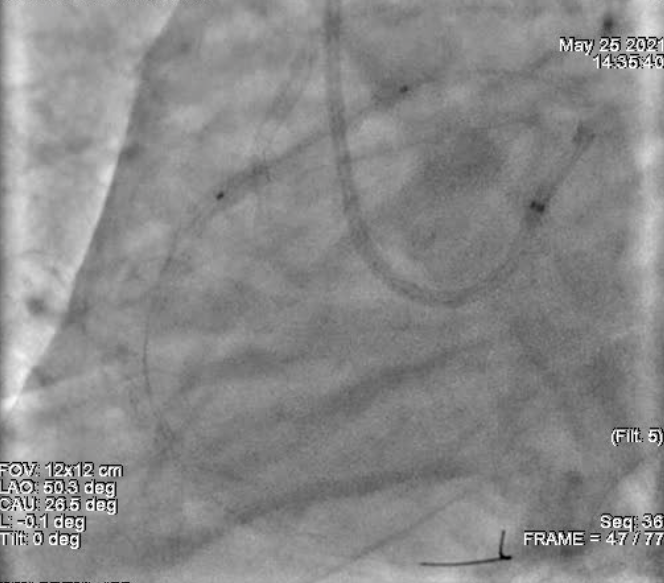
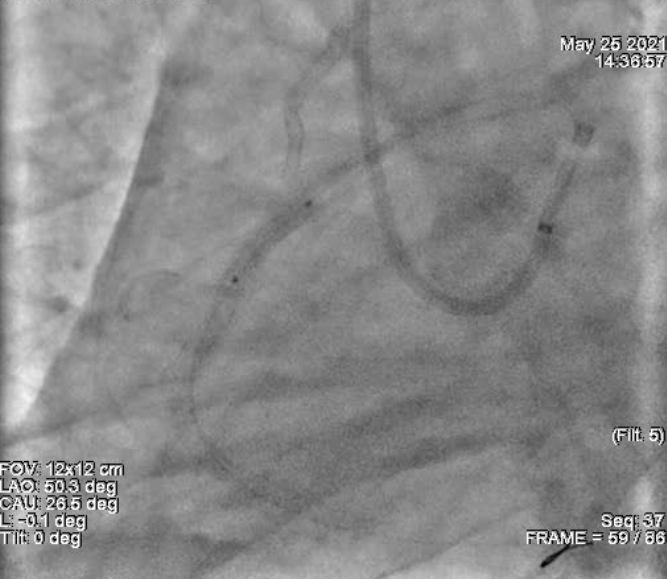
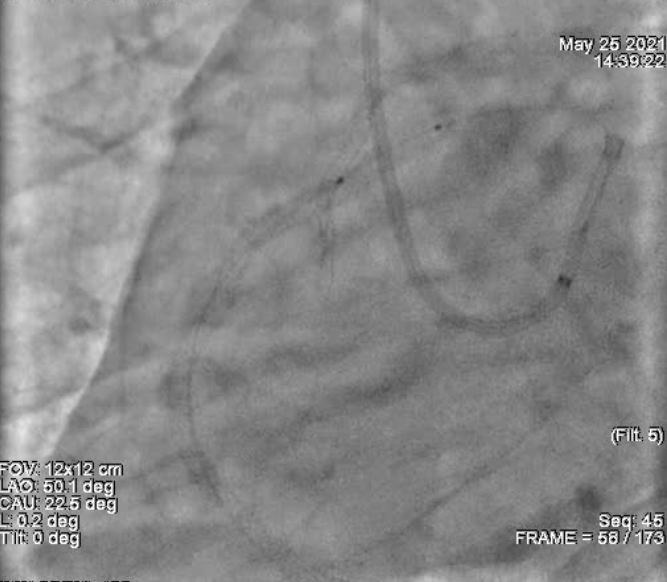
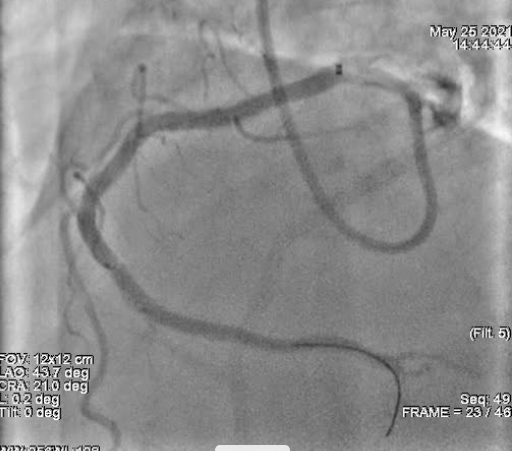
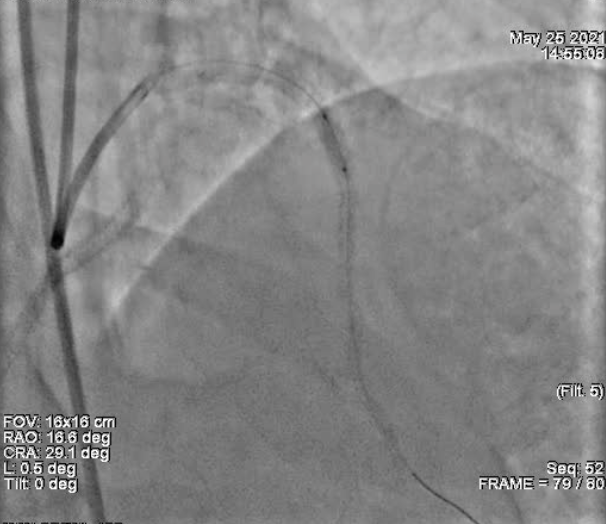
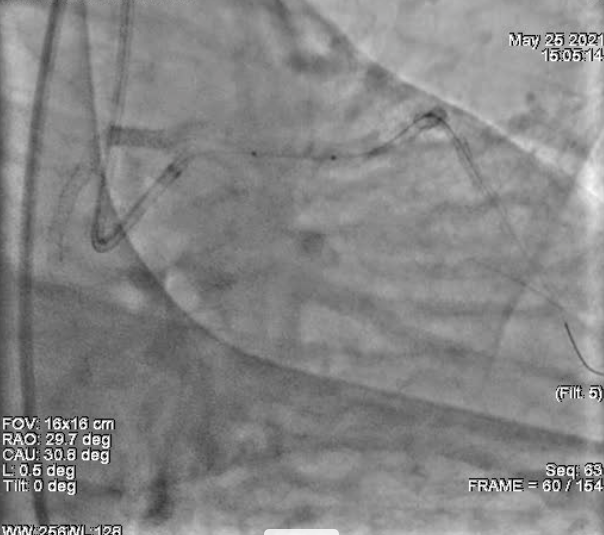
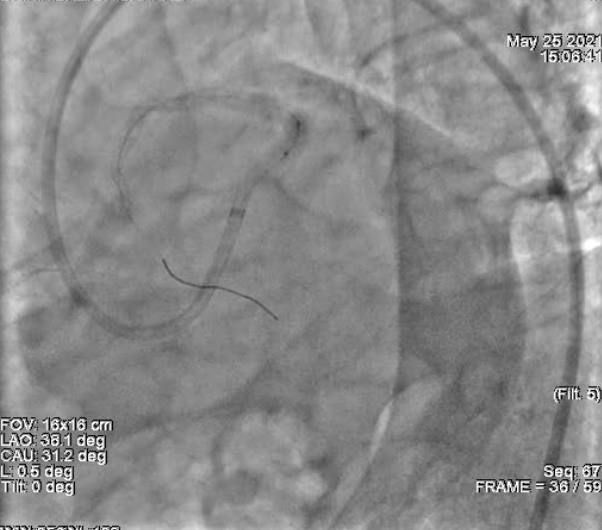
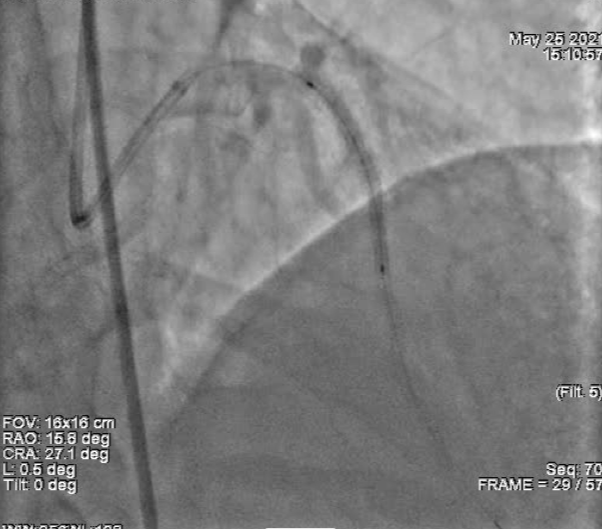
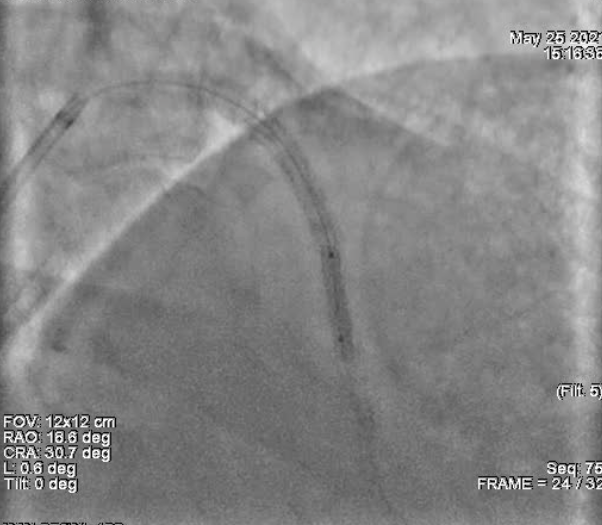
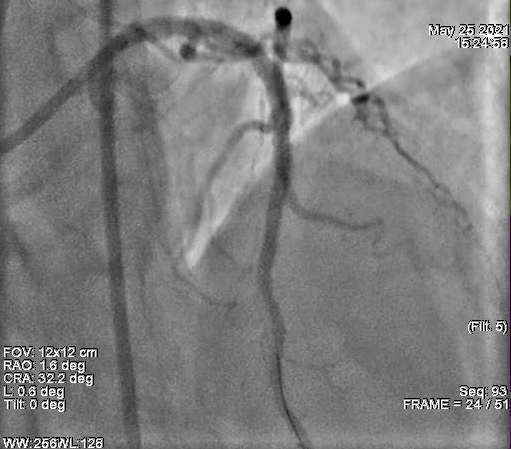
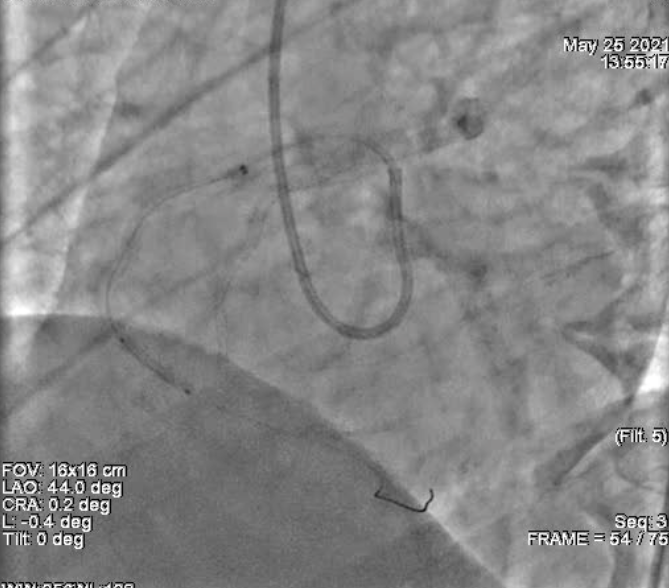
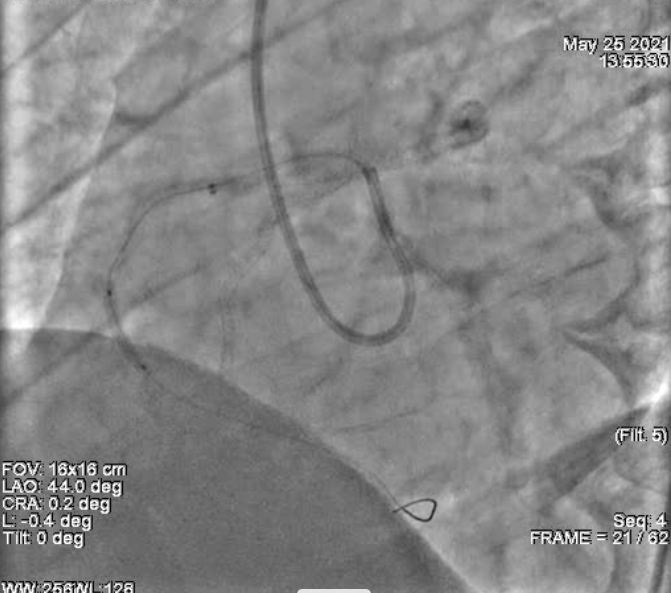
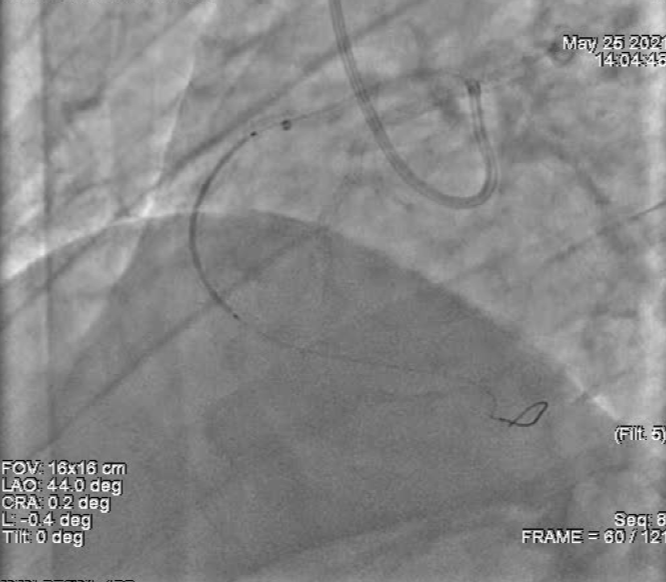
LM: Normal LAD: Type III vessel, Proximal segment discrete lesion with ISR of 80% . mid segment discrete ISR of >90%. Diagonal: Normal LCx: Non-dominant, normal. OM: OM1-normal, OM2- proximai segment 60-70% stenosis (small calibre vessel) RCA: Dominant. anomalous origin frorn left coronary sinus. Mid segrnent calcific vessel with 90% stenosis. PDA: Normal PLV: Normal




Interventional Management
Procedural Step
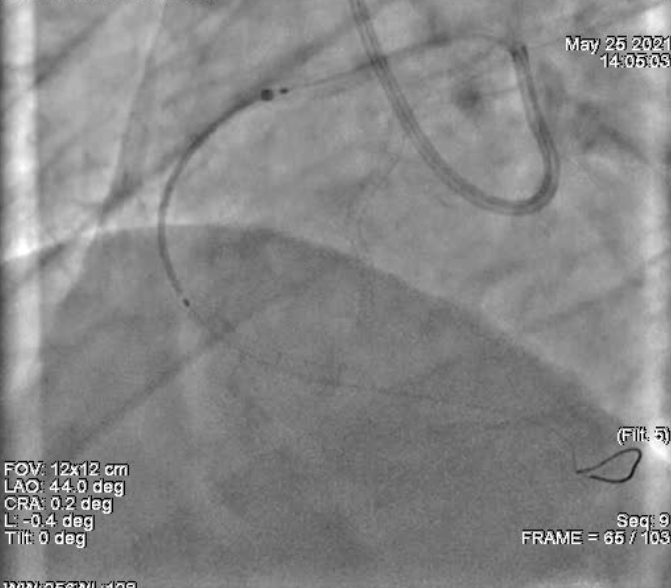
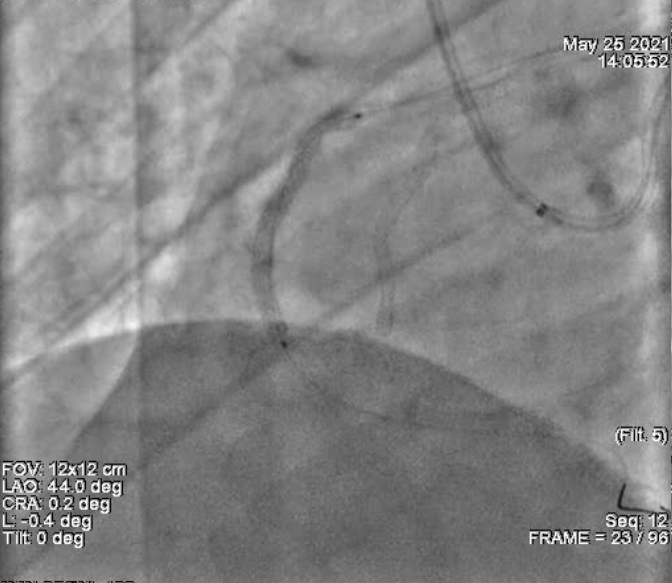
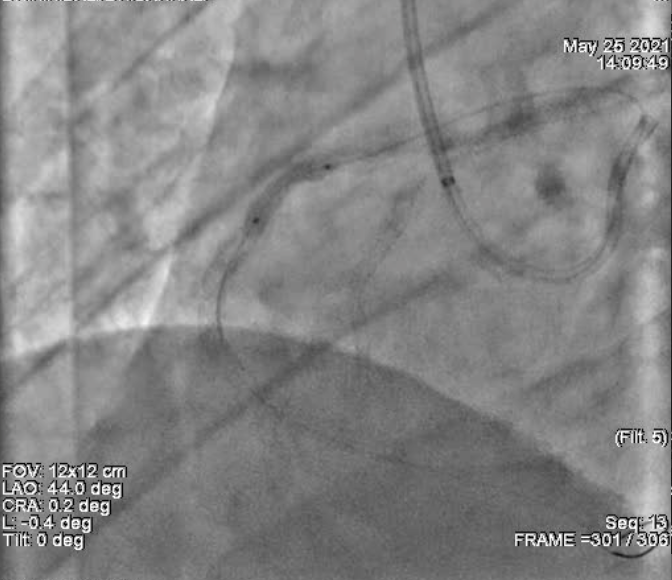
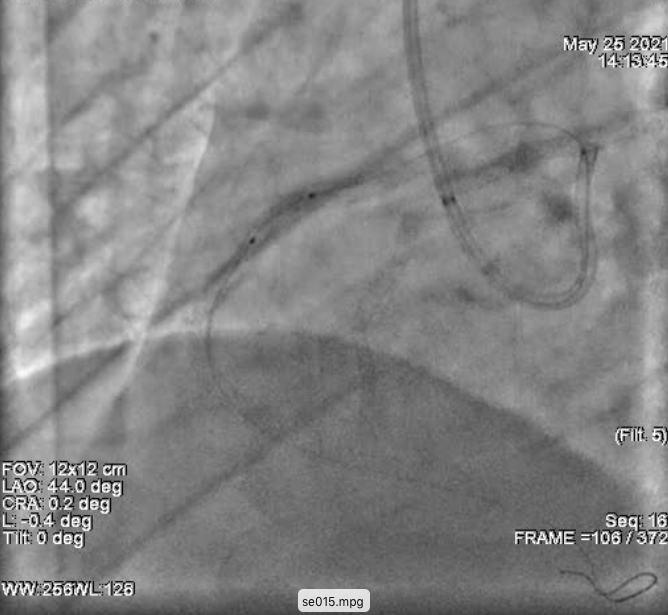
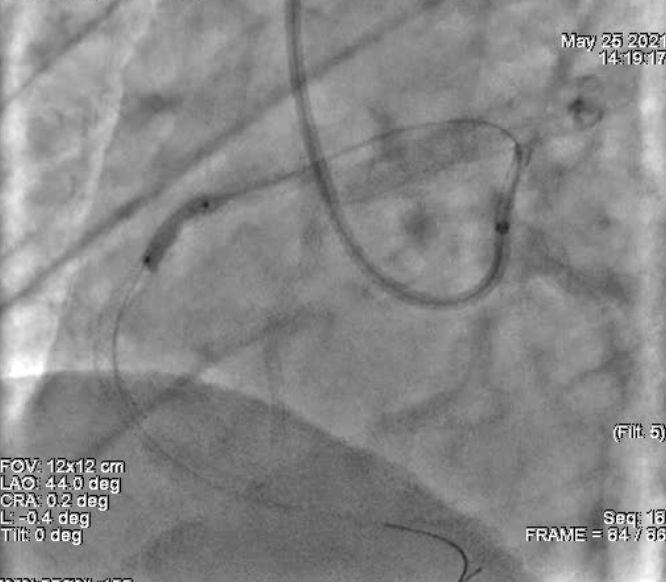
PTCA and stent to anomalous RCA & LAD ISR done throught the Right femoral arterial route. Guiding catheter: 7F EBU 3.5, 6F AL 1 Guding wire: BMW Additional hardware used: Guideliner 6F, OPN NC 2.5x10 mm, Shockwave 3.0x 12mm 3 overlapping stents deployed in proxinmal to distal RCA, 2 overlapping stents deployed in proximal to distal LAD Pre stent diiatation done with 2.5x15mm balloon Post stent dilatation done with 2.5x15mm, 2.75x15mm, 3.0x 12mm, 3.5x 12mm NC balloon





Case Summary
Intravascular lithotripsy is a relatively new technique for management of heavily calcified coronary artery lesions. We report a case in which IVL was done in two vessels in the same sitting, in an anomalous RCA for underdeployed stent and in LAD for ISR.