
CASE20210823_002
CTO Intervention with Minimal Contrast Usage Using Coronary Imaging ( IVUS )
By , , , , , , ,
Presenter
Vijayendran Rajalingam
Authors
1, 1, 1, 1, 1, 1, 1, 1
Affiliation
, Malaysia1
Imaging - Invasive Imaging (IVUS, OCT, spectroscopy, etc)
CTO Intervention with Minimal Contrast Usage Using Coronary Imaging ( IVUS )
1, 1, 1, 1, 1, 1, 1, 1
, Malaysia1
Clinical Information
Patient initials or Identifier Number
Mr K
Relevant Clinical History and Physical Exam
56 year old Chinese male History Of Bilateral Hydronephrosis with Bilateral proximal Ureteric Calculus as part of pre operation optimization he was Referred to Cardiology team in view of ECG Changes ( attached ) Further history complain of reduce effort tolerance off recently o/e
 4CH echo pre coros .mov
4CH echo pre coros .mov
plax pre coros.mov
Relevant Test Results Prior to Catheterization
ECG : LBBB , early transition at v3,v4 , inferior axis
HOLTER : > 30%
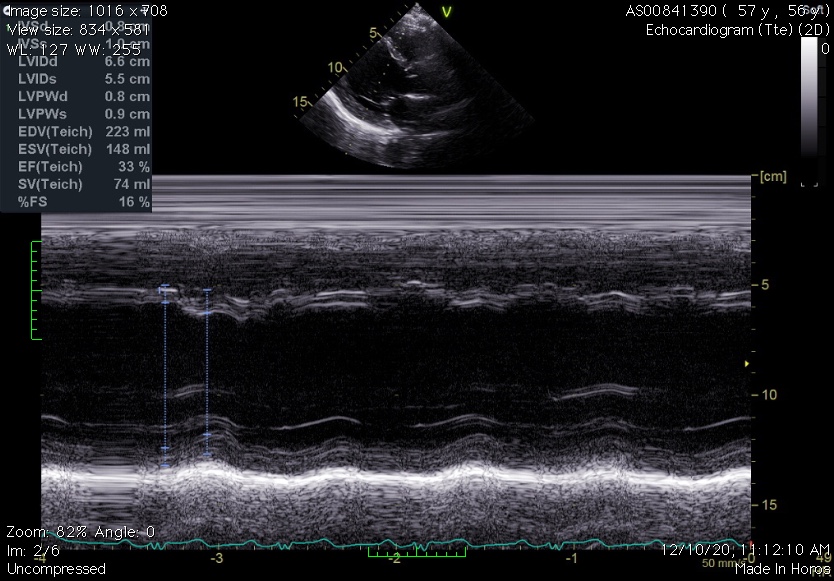
ECHO : EF 33% GLOBAL HYPOKINESIA RWMA PRESENT
HOLTER : > 30%
ECHO : EF 33% GLOBAL HYPOKINESIA RWMA PRESENT
Relevant Catheterization Findings
LEFT SYSTEM :
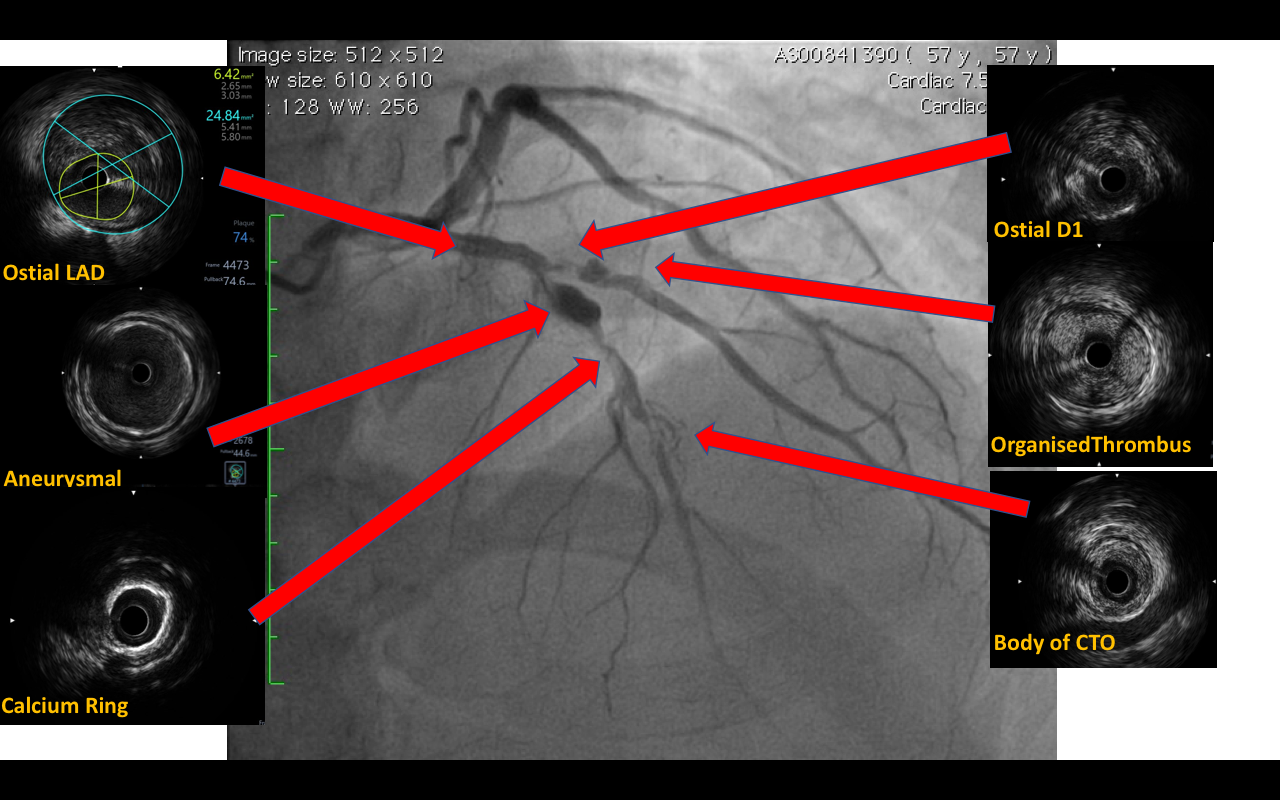
Left Main system normal Proximal LAD 60- 70% stenosis mid LAD CTO with prestenotic aneurysmal segmentDiagonal 1 ostium 95% stenosis with post stenotic aneurysmal segment
Right SYSTEM:
Ectatic Right Coronary System proximal PLV 80%
diagnostic cag ( spider ).mov
diagnostic CAG.mov
diagnostic lao:cra.mov
diagnostic RAO Cau.mov
diagnostic rca cra.mov
diagnostic rca lao.mov
dianostic RCA.mov
Left Main system normal Proximal LAD 60- 70% stenosis mid LAD CTO with prestenotic aneurysmal segmentDiagonal 1 ostium 95% stenosis with post stenotic aneurysmal segment
Right SYSTEM:
Ectatic Right Coronary System proximal PLV 80%
Interventional Management
Procedural Step
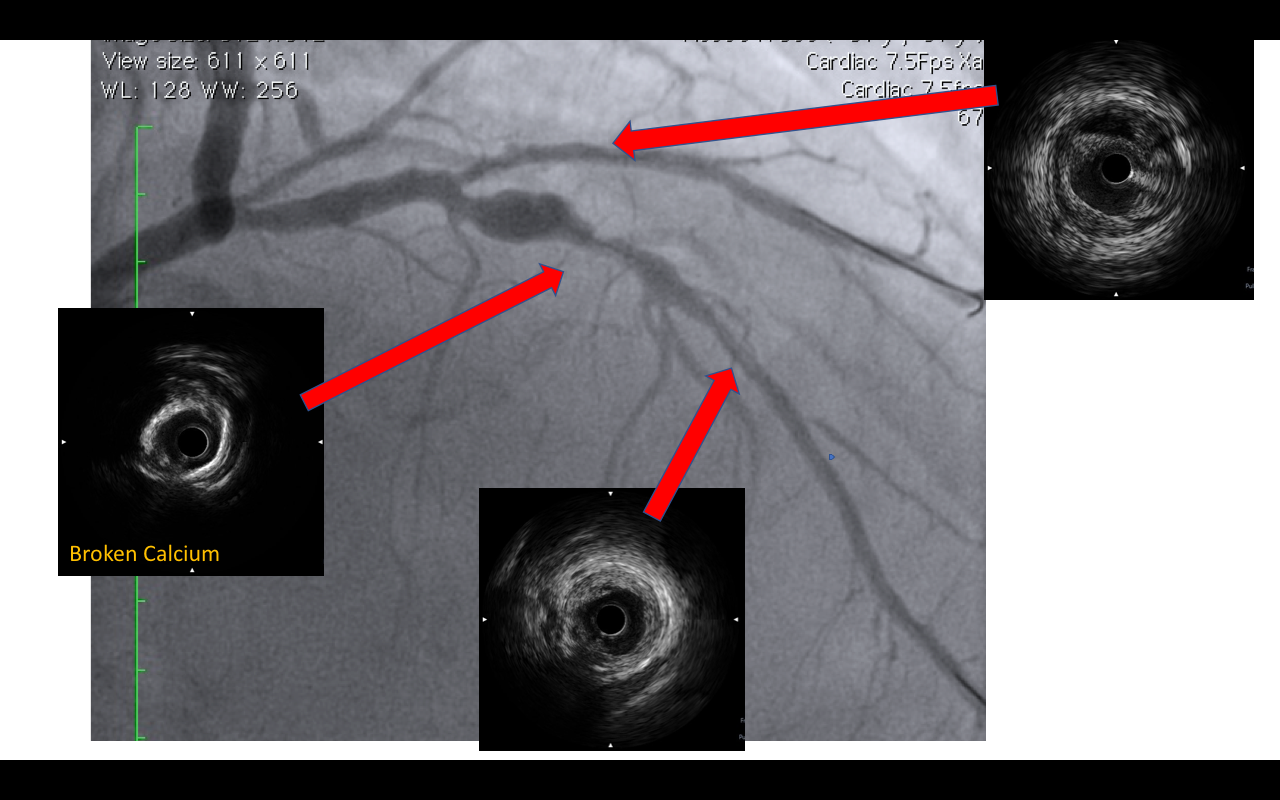
Procedural steps : 1) EBU 3.5 , 7 Fr
Cross CTO LAD .mov
Wired D1 with fielder XTR.mov
crossed with gaia 1st .mov
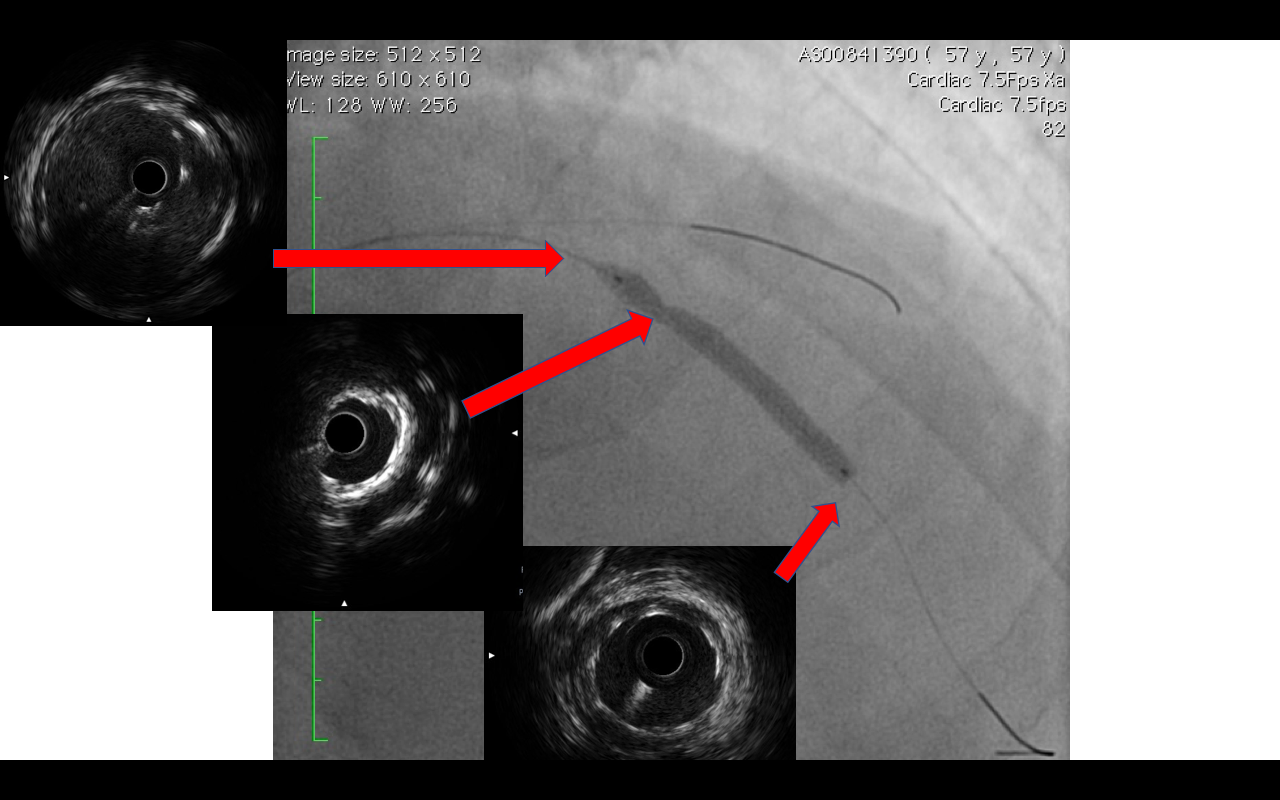
FINAL ANGIO .mov
Case Summary
Post CAG - No complication total contrast used 45 cc
Post angiography ECG : normal sinus rythm ( Resolutions of PVCs ) Repeated HOLTER PVC burden < 1 %ECHO improved in LV function 40%
Patient remains well Plan for relook 9 months
Post angiography ECG : normal sinus rythm ( Resolutions of PVCs ) Repeated HOLTER PVC burden < 1 %ECHO improved in LV function 40%
Patient remains well Plan for relook 9 months