
CASE20210825_001
Ultra Low Contrast Unprotected Left Main Percutaneous Coronary Intervention Using Intravascular Ultrasound and Sepal Technique
By , , ,
Presenter
Kristy Garganera
Authors
1, 1, 1, 1
Affiliation
, Philippines1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Ultra Low Contrast Unprotected Left Main Percutaneous Coronary Intervention Using Intravascular Ultrasound and Sepal Technique
1, 1, 1, 1
, Philippines1
Clinical Information
Patient initials or Identifier Number
BK
Relevant Clinical History and Physical Exam
A 60 year old male hypertensive, diabetic with CKD stage 4 presenting with easy fatigability managed as a case of ischemic cardiomyopathy referred for coronary intervention. At the ER his vital signs are as follows: BP 110/70mmHg, HR 71bpm, RR 20cpm. Pink palpebral conjunctiva, non-engorged neck veins, clear breath sounds, apex beat at 5th intercostal space mid axillary line with no murmur, good peripheral pulse with grade 1 bipedal edema.
Relevant Test Results Prior to Catheterization
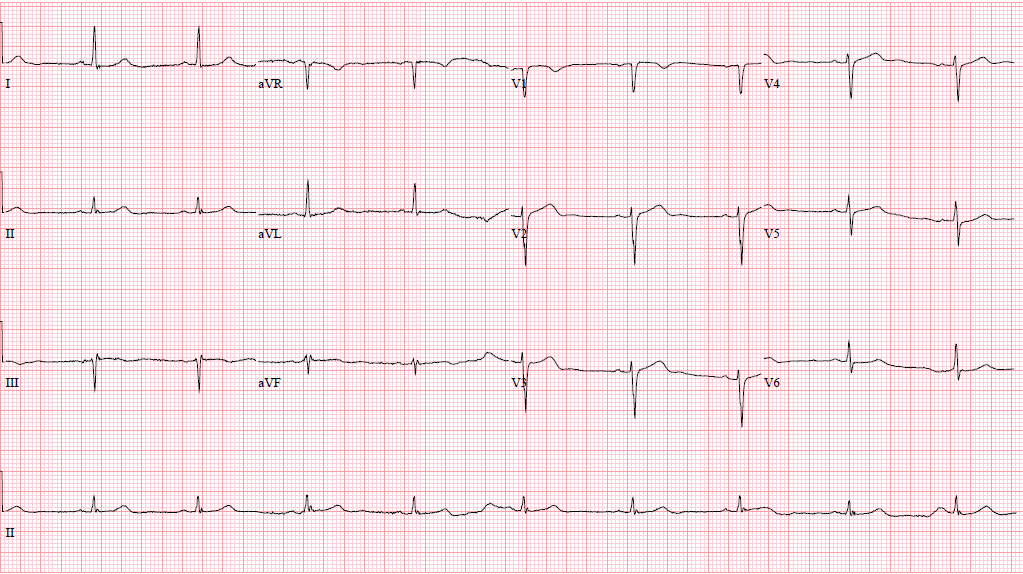
12 lead ECG revealed sinus bradycardia with poor R wave progression. Chest Xray AP view showed no significant chest findings. Creatinine at 251.40 umol/L and an eGFR of 23, Uric Acid at 565.90 umol/L, and HbA1c of 9.3.
Relevant Catheterization Findings
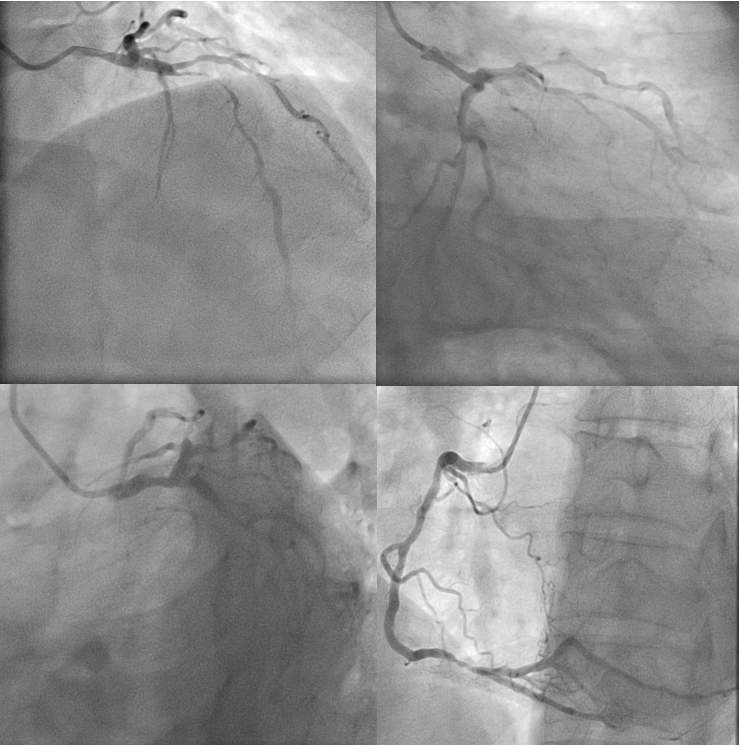
LMCA is a 4.0mm vessel with 65% mid to distal segment stenosis. It bifurcates into the LAD and LCx. LAD is a 3.5mm type III vessel with long 90-95% proximal to mid segment stenosis, the distal segment has mild myocardial bridging. LCx is a 3.0mm vessel with 30-40% mid segment stenosis and a 20% distal segment stenosis. RCA is a 4.0mm dominant vessel with a 70-80% distal segment stenosis just before the crux.
 BK RAO CRANIAL.avi
BK RAO CRANIAL.avi
BK LAO CAUDAL.avi
Interventional Management
Procedural Step
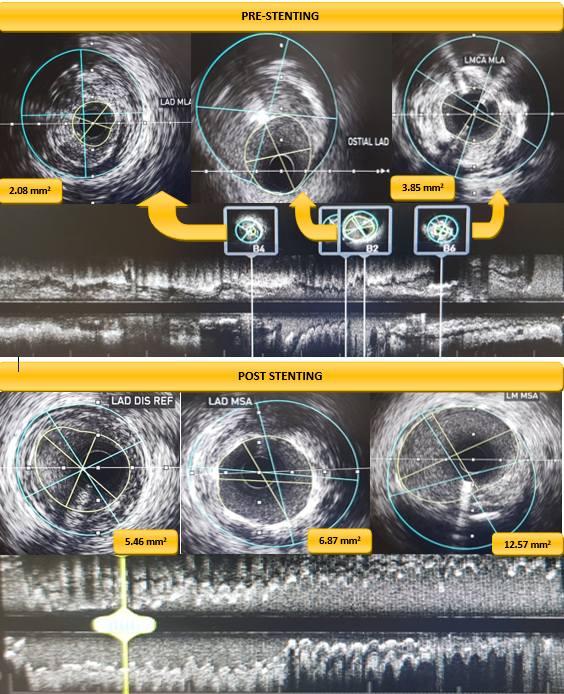
Using right radial access, 7F guide catheter, and previous angiogram for mapping, coronary wires were distalized to the LAD, LCx, and D1.IVUS show concentric fibrofatty plaque in LAD with MLA of 2.08mm2,distal reference 5.46mm2,LMCA show concentric mixed plaque with MLA of 3.98mm2.Predilation from mid LAD to proximal LMCA using 2.0x20mm compliant balloon at 14-20ATM.Repeat IVUS warranted more predilation thus a 2.50x15mm compliant balloon dilation from the mid LAD to proximal LMCA at 14-20ATM.DES 3.0x38mm placed at proximal to mid LAD and deployed at 11ATM.Stent balloon used to postdilate at 15ATM.To guide in ostial stent placement,sepal wire technique was done using the diagonal wire.Second DES 4.0x38mm positioned at the proximal LAD to aorto-ostial segment with 4mm distal overlap from first stent and deployed at 11ATM.POT of LMCA using 5.0x8mm NC balloon at 12ATM.Partial strut distortion noted when jailed LCx wire pulled out and guide catheter was pulled in.Postdilation with 3.0x15mm compliant balloon of proximal LMCA to aorto-ostial area at 10-16ATM.IVUS show stent underexpansion at mid LAD with partial stent distortion in aorto-ostial area.Postdilation with 3.5x20mm NC balloon at mid LAD at 18ATM.NC 5.0x8mm balloon inflated in aorto-ostial area at 12ATM.IVUS show complete stent apposition,no dissection,LAD MSA 6.87mm2 and LMCA MSA 12.57mm2 with plaque burden <50%.Post angiography no residual stenosis/perforation with TIMI 3 flow.Total of 10ml iso-osmolar contrast used.
BK SEPAL WIRE TECHNIQUE.avi
BK FINAL ANGIOGRAM.avi
Case Summary
With proper planning, IVUS-optimized ultra low contrast PCI of unprotected LM with crossover stenting to LAD is feasible and can be safely done especially in patients who are at high risk for having contrast induced nephropathy. IVUS was vital for assessment of vessel diameter, plaque morphology, adequacy of lesion preparation, stent sizing and length, and apposition of stent struts to vessel wall. Coronary wires were used as visual guides as to where we positioned our balloons and stents coupled with IVUS and strategies such as the sepal wire technique for aorto-ostial LMCA stenting to avoid geographic miss.