
CASE20210825_003
High Risk Rotational Atherectomy in Uncrossable Long and Heavily Calcified Lesion in Elderly Patient with Unstable Ventricular Tachycardia / Atrial Fibrillation
By , , ,
Presenter
Quah Wy Jin
Authors
1, 1, 1, 1
Affiliation
, Malaysia1
Complex PCI - Calcified Lesion
High Risk Rotational Atherectomy in Uncrossable Long and Heavily Calcified Lesion in Elderly Patient with Unstable Ventricular Tachycardia / Atrial Fibrillation
1, 1, 1, 1
, Malaysia1
Clinical Information
Patient initials or Identifier Number
MSW
Relevant Clinical History and Physical Exam
75 years old gentleman underlying Diabetes Mellitus and Hypertension presented with angina and palpitations. Treated for NSTEMI in failure and had recurrent atrial fibrillation in rapid ventricular response needing synchronized cardioversion. This was his first admission.
Relevant Test Results Prior to Catheterization
12 lead ECGs showed atrial fibrillation in rapid ventricular response (up to 160 beats per minute) before reverting to sinus rhythm and deep T wave inversions at V1 - V5.Echocardiography showed left ventricular ejection fraction of 40% but no significant valvular lesions.Haemoglobin was 10.2 g/dl (normochromic normocytic picture). Troponin was raised at 16 pg/ml. NT-proBNP was 3375 pg/ml. HbA1c was 6.2%.
Relevant Catheterization Findings
Diagnostic coronary angiogram showed mild disease at distal left main. There was a severely stenotic (>90%) long and heavily calcified lesion from the ostium till mid segment of the left anterior descending artery. The left circumflex artery was dominant and normal. The right coronary artery was small, non dominant and had diffuse disease.
 Diagnostic Coronary Angiogram (Spider view).mpg
Diagnostic Coronary Angiogram (Spider view).mpg
Diagnostic Coronary Angiogram (Cranial view).mpg
Diagnostic Coronary Angiogram (RCA).mpg
Interventional Management
Procedural Step
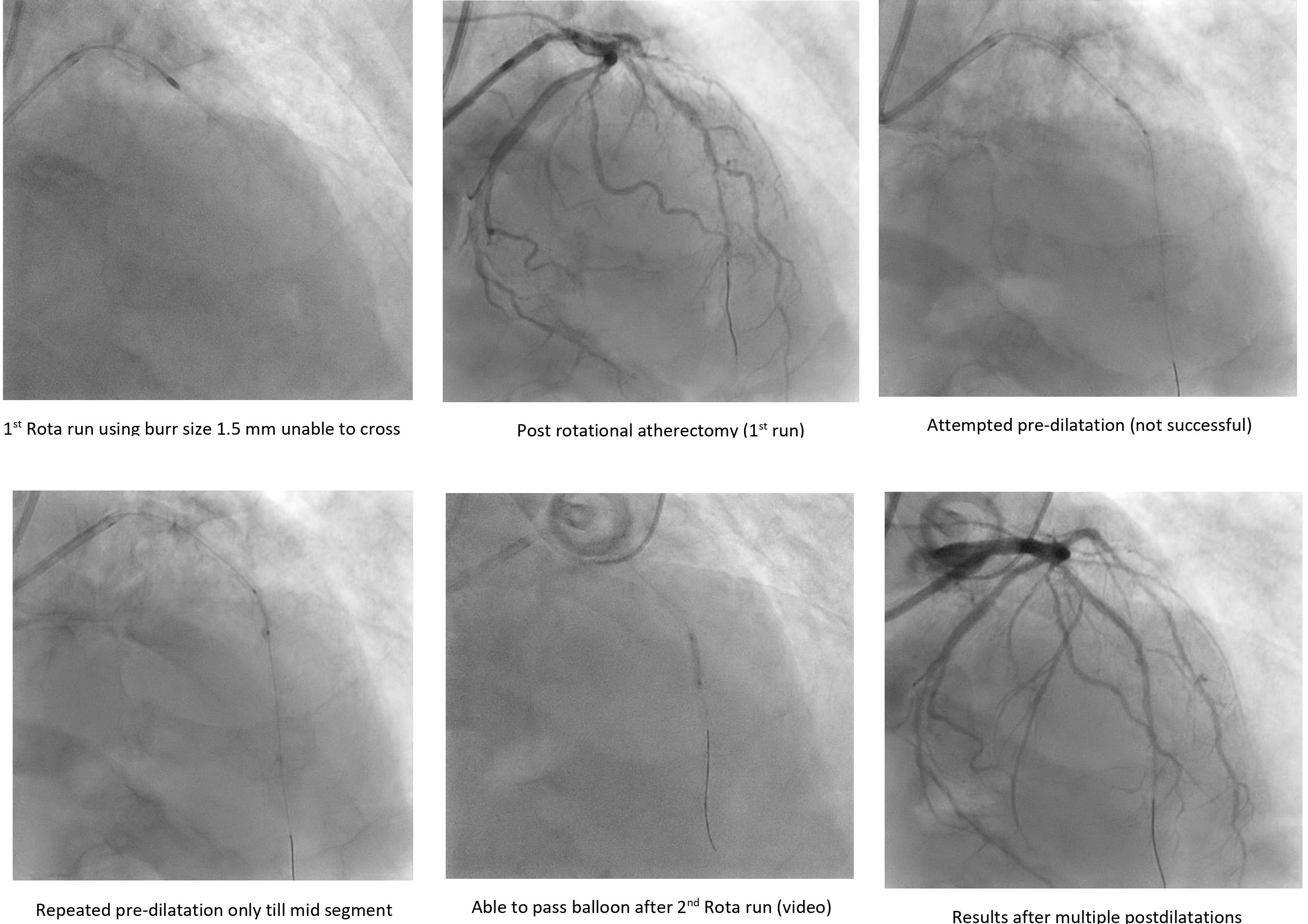
After discussion with the family, the decision was to proceed for high risk PCI to the LAD with rotational atherectomy. Trans-radial approach was employed using Glidesheath Slender 7Fr. An EBU 3.5/7Fr guiding catheter was used. In view of the tight lesion, a finecross microcatheter was used with Sion Blue guidewire to cross the lesion. Wire trapping technique used to exchange to a Rota-Floppy guide wire. A single Rota Burr size of 1.5mm was used with speed of 160000 rpm. However, unable to pass the mid -segment and patient went into unstable monomorphic VT requiring synchronized cardioversion of 200J. Then attempted to predilate with a NC 2.0 X 15mm up to 24 atm but still unable to open fully. Decided for another run using the same Rota Burr size of 1.5mm at 170000 rpm. Managed to cross tightest mid segment lesion. Wire exchanged back to Runthrough Floppy (workhorse wire). Predilated with NC Emerge 2.0 X 15mm till high pressures of 26 atm and was successful. Proceeded then with NC Scoreflex 2.5 X 15mm till 20 atm and NC Emerge 3.0 X 15mm till 20 atm. Patient intermittently required electrical cardioversion under sedation for unstable VT / AF. Proceeded with stenting of mid-segment of LAD with SYNERGY 2.5 X 32 mm and proximal segment till ostium LAD with SYNERGY 3.0 X 28mm. Post dilatation with NC Emerge 3.0 X 15mm till 22 atm. TIMI 3 flow was established and patient's haemodynamics improved. No stent edge dissections were seen angiographically.
2) Crossing with Rotational Atherectomy.mpg
3) Final result.mpg
Case Summary
This complex case demonstrates the effectiveness of rotational atherectomy in approaching an uncrossable long calcified lesion. Based on ARC-HBR, he has 4 major criteria and 1 minor criteria, hence he is of high bleeding risk. As patient was haemodynamically unstable and due to financial constraints, we were unable to use intravascular imaging and had only 1 size of Rota Burr at our disposal. Therefore, planning is crucial and every step of the intervention had to be quick and smooth. The procedure was successful and patient was discharged well after few days of monitoring in ward.