
CASE20210828_001
Accidental STAR with Ellis III Perforation in VF Arrest Primary PCI
By
Presenter
Jonathan Fang
Authors
1
Affiliation
, Hong Kong, China1
Complications - Complications
Accidental STAR with Ellis III Perforation in VF Arrest Primary PCI
1
, Hong Kong, China1
Clinical Information
Patient initials or Identifier Number
DB
Relevant Clinical History and Physical Exam
64 year-old man collapsed on the street with bystander CPRFound to be VF arrest. Defibrillation on ambulance 5 timesRefractory VF with ECMO inserted at the emergency department and commenced E-CPR with established 45 minutes after onset of symptomEcho LVEF 25% global hypokinesiaSent to Cath lab for primary PCI
Relevant Test Results Prior to Catheterization
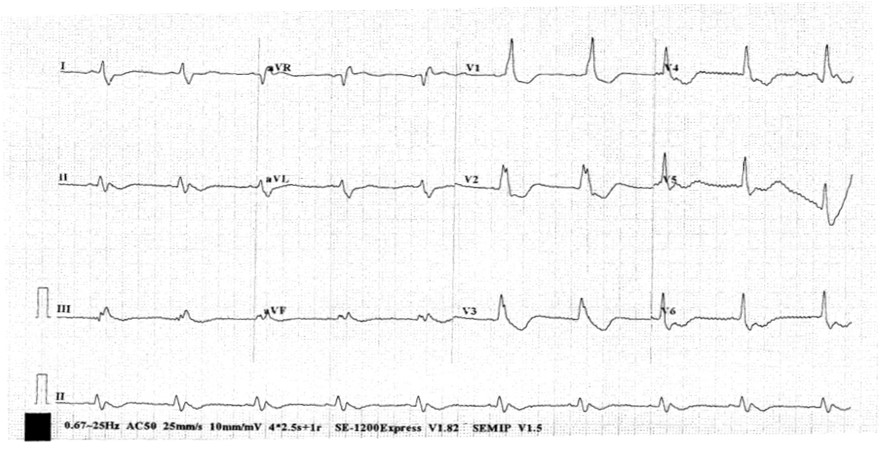
ECG RBBB and diffuse TWI
Relevant Catheterization Findings
pRCA occluded LM-LAd 40% dsLCx ostial CTO. OM filled by L->L collaterals
 Media1.mp4
Media1.mp4
Media2.mp4
Media3.mp4
Media4.mp4
Media5.mp4
Interventional Management
Procedural Step
VA ECMO via RFA RFV
Media6.mp4
Media7.mp4
Media8.mp4
Media9.mp4
Media10.mp4
Media11.mp4
Media12.mp4
Media13.mp4
Media14.mp4
Media15.mp4
Media16.mp4
Media17.mp4
Media18.mp4
Media19.mp4
LFA 6Fr access. JR4 guide
Sion Blue GW encountered difficulty when wiring. Wired with knuckling
p-mRCA predilation with 3.0/12 balloon followed by thrombus aspiration with penumbra for 2 passes
pRCA stent with 4.0/38 DES at 12atm and postdilate with 4.0x15 NC balloon at 12atm
Noted filling defect distal to stent. IVUS done followed by stent with 4.0x22 DES at 10atm
Post stenting noted Ellis class 3 perforation at stent overlap segment. Immediate balloon tamponade followed by reassessment after 15 and 30 imnutes. Persistent extravasation. Cover stent (PK Papyrus) 4.5 x 20m and 3.5x 15 followed by further balloon occlusion. Pericardiocentesis done with access with micropuncture set with 0.18 peripheral wire and upsizing to pericardiocentesis set. Further balloon occlusion with 4.0 stent balloon. No further extravasation
IVUS showed that the p-dRCA segment was actually in the suboptimal space and there was subintimal tracking with disseciton-reentry ( STAR) in distal RCA PDA/PL bifurcation.
Case Summary
In acute cardiac arrest setting with primary PCI, inadvertent wiring into subintimal space could occur
Intra-vascular imaging is important for troubleshooting
Consider downsizing when in subintimal space