

POT Useful for All Bifurcation PCI Lesions in PCI; Final Kissing Balloon Needed After 1-Stenting?
Both techniques should tailor to anatomy but data on optimized KBT with POT still missing
Proximal optimization technique (POT) with strategic employment of the kissing balloon technique (KBT) can help avoid opening the PandoraĄŊs box of complications related to a compromised side branch (SB) in bifurcation lesions, an expert said.
 Alaide Chieffo, MD (San Raffaele Scientific Institute, Milan, Italy) at COMPLEX PCI 2021 Virtual on Nov. 25 highlighted the usefulness of POT in bifurcation lesions, the potential of KBT in single stenting, and the necessity of tailoring stents to anatomy.
Alaide Chieffo, MD (San Raffaele Scientific Institute, Milan, Italy) at COMPLEX PCI 2021 Virtual on Nov. 25 highlighted the usefulness of POT in bifurcation lesions, the potential of KBT in single stenting, and the necessity of tailoring stents to anatomy.
Ą°POT is useful for all bifurcation lesions since distal vessel sizing limits carina shift according to the 1-stent, 2-diameters concept. KBT may be useful after single stenting and necessary in certain cases like XX0 lesions although the clinical validation of optimized KBT on top of POT is still missing,Ąą Chieffo said.
POT and KBT are both techniques used to limit the risk of SB compromise by tailoring a regular stent into a Ą°dedicatedĄą one. The methods rely on the mechanisms of the carina shift and longitudinal plaque shift in the proximal left main (LM) vessel.
Evaluations suggest a benefit from the new kissing balloon technique, need for final POT, and competition between POT/Side/POT vs. POT/Kiss/POT.
Provisional single stenting and upfront two-stenting are two strategies to treat bifurcation lesions in percutaneous coronary intervention (PCI). Bifurcation lesions, which account for up to 20 percent of all PCI cases, are harder to treat and have a higher procedural complication rate and risk of long-term adverse events.
Although KBT is a default procedure with the upfront two-stent strategy, conflicting study results have shown KBT in stepwise provisional stenting could cause complications in an already long and complicated procedure.
The NORDIC III1 study examining KBT versus non-KBT in bifurcation lesions after stepwise provisional stenting reported no significant differences between the two arms - although subanalysis showed benefits with the final kissing balloon technique (FKT).
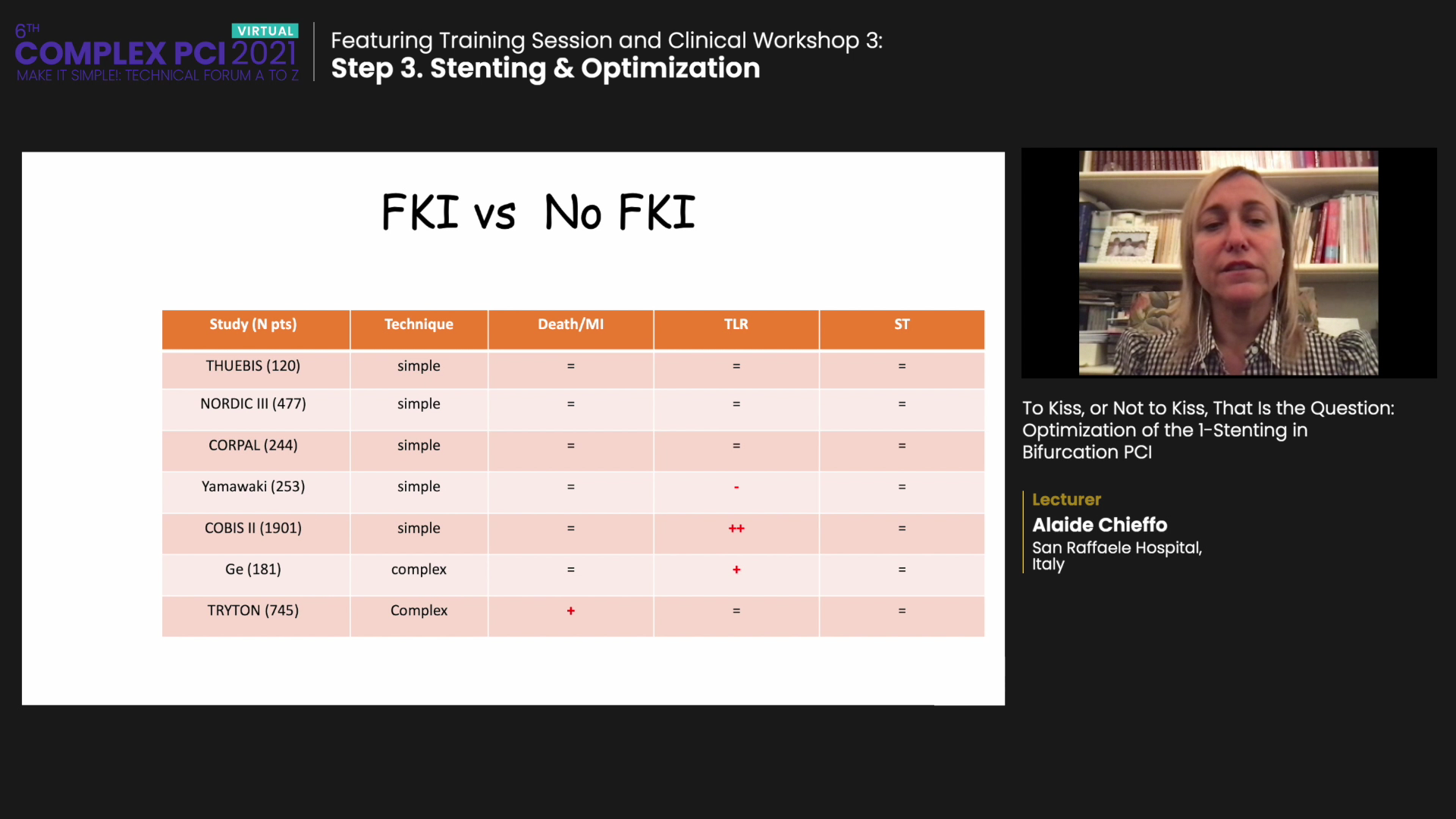
Analysis of seven studies that examined FKT versus non-FKT - including THUEBIS2, NORDIC III, COBIS II3, and others - also demonstrated no significant difference between the two strategies. The only study slightly favoring FKT was COBIS II. Subanalysis of the RAIN-CARDIOGROUP VII Registry4 evaluating LM bifurcations also showed no benefits of FKT versus non-FKT for major adverse cardiovascular events (MACE), death, myocardial infarction (MI), or stent thrombosis.
Although questions remain, Chieffo pointed out that optimizing FKT requires a combination of distal cell wiring, non-compliant (NC) balloons sized to the distal reference, and minimal overlap.
On the other hand, POT can be helpful in all cases to ensure full dilation of the proximal segment. Ą°Distal main branch sizing employed to conform the main branchĄŊs stent to the distal reference can help prevent distal shift while POT helps ensure full dilation of the proximal segment,Ąą she said.
Advantages of POT have been demonstrated in several studies, including COBIS II subanalysis, E-ULTIMASTER5, and NORDIC III.
Subanalysis of the COBIS II trial that only included patients with a side branch diameter ĄÃ2.5 mm showed POT (compared to non-POT) had a lower MACE occurrence driven mainly by lower rates of target lesion revascularization.
The E-ULTIMASTER registry on 1,168 bifurcation lesions confirmed benefits of POT by demonstrating lower MACE occurrence in the target lesion, revascularization of target vessel failure, and stent thrombosis.
NORDIC III further demonstrated the benefits of provisional POT in provisional side branching. The main advantages included more side branch opening to prevent peri-procedural occlusion (non-Q-wave MI), relief of angina, and continued open access for future interventions.
The potential pitfall of POT is SB fenestration, Chieffo said, which can lead to stent distortion and call for KBI.
Where to place the stent is crucial for POT. The stent should be placed proximally enough to allow for balloon inflation without contacting the bifurcation. POT should be performed before wire exchange and according to the size of the NC balloon (shoulder and marker).
Chieffo recommended sizing by proximal reference (1:1) with the distal marker at the level of the carina and selecting a view with the maximal angle to avoid overlap. Ą°Overall, bench and virtual evaluations suggest a benefit from the new kissing balloon technique, need for final POT, and possible competition with POT/Side/POT versus POT/Kiss/POT.Ąą
- https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.110.966879
- https://www.ahajournals.org/doi/10.1161/CIRCINTERVENTIONS.108.833046
- https://www.jacc.org/doi/abs/10.1016/j.jacc.2013.07.041
- https://www.ahajournals.org/doi/10.1161/CIRCINTERVENTIONS.119.008325
- https://www.terumo-europe.com/en-emea/clinical-evidence/e-ultimaster-trial