
CASE20220812_001
My first OCT guided PCI for STEMI as a junior
By
Presenter
Chun Lin Raymond Cheung
Authors
1
Affiliation
, Hong Kong, China1
Imaging - Invasive Imaging (IVUS, OCT, spectroscopy, etc)
My first OCT guided PCI for STEMI as a junior
1
, Hong Kong, China1
Clinical Information
Patient initials or Identifier Number
HM Chan
Relevant Clinical History and Physical Exam
Our patient is Mr Chan, a 68 year old retired driver. He is a chronic drinker, 40 pack years, and a social drinker.
He has a medical history of diabetes and hyperlipidemia.
He complained of sudden onset of severe chest pain at 12 midnight on 27/7/200 whilst watching TV.
Vitals were stable on admission. He was not in heart failure. Physical exam was unremarkable.
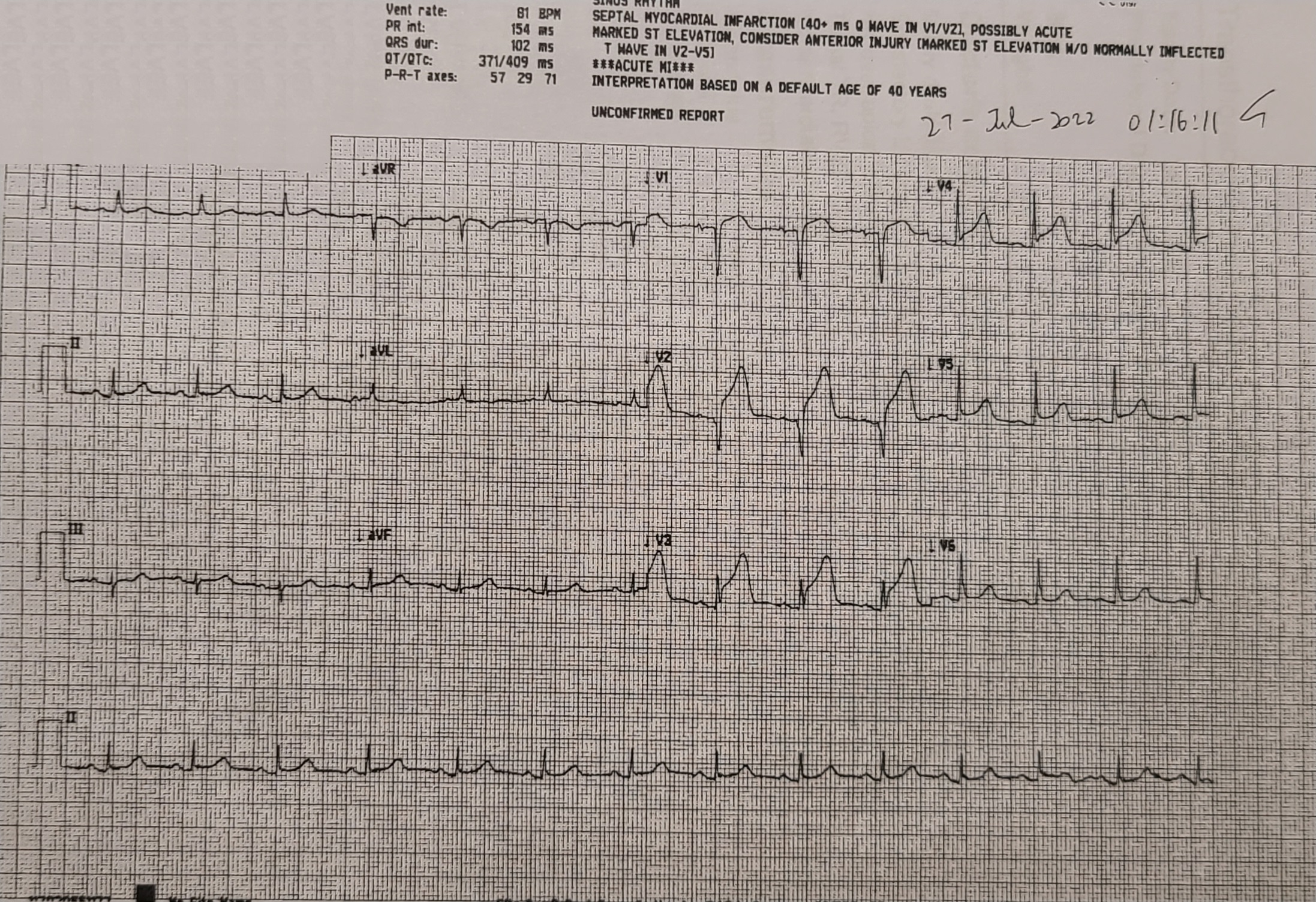
ECG showed SR, ST elevation at leads V2-5, suggestive of anterior STEMI.
Relevant Test Results Prior to Catheterization
He was treated with thrombolytics, sent to CCU, and planned for PCI the next day. CXR was clear.Blood tests showed normal complete blood count, liver and renal function test. troponin and CK were elevated. Echo showed normal LV size and systolic function, EF 51%, hypokinesia at apical and anterior wall. There was no pericardial effusion.
 echolax.avi
echolax.avi
echo4ch.avi
echosax.avi
Relevant Catheterization Findings
The patient was sent to catherization lab for pharmacoinvasive PCI the next day morning. Diagnostic coronary angiogram was performed via right radial access with JL4 & JR4. LMS: minor diseaseLAD: p-mLAD critical disease, TIMI III flow LCX: dLCX 30% diseaseRCA: minor irregularities, dominant
leftcaudal.mp4
leftcranial.mp4
rca.mp4
Interventional Management
Procedural Step
The culprit vessel is LAD, compatible with ECG. Decided for PCI to LAD.The Left main was engaged with JL3.5 7Fr. LCX was wired with NS runthrough for protection.LAD was wired with Fielder FC. p-mLAD was first predilated with Ryurei 2.0/15 at up to 16atm. Dragonfly Opstar OCT with Ultreon was used for lesion sizing, characteristics and landing. Xience 2.5/38 was deployed at at mLAD at 12atm. Xience 3.5/28 was deployed at at pLAD at 12atm with stent overlapping. NC trek 2.5/15 was used for stent dilatation at up to 20atm. The pLAD stent was then post dilated with NC trek 3.5/15 at 18atm. Angiographic result was good apparentlyBut OCT was used again and showed mild underexpansion at mLAD stent. mLAD stent was post dilated again with NC trek 3.0/12 at up to 16atm. OCT finally showed improve apposition.Final angiogram showed TIMI III flow with no acute complication.

finalshot.mp4
stenting.mp4
stenting2.mp4
Case Summary
OCT guided PCI to LAD was performed successfully. The patient was discharged 3 days later with no chest pain. This case may present one of the day in day out cases commonly encountered in cath lab, but it was the first STEMI case that I was allowed to be the chief operator as a cardiology trainee. Live procedure video was recorded with simultaneous fluoroscopic images and pressure tracings. Luckily I could perform this case uneventfully from diagnostic coronary angiogram, wiring, OCT, to balloon dilatation and stenting, despite a longer time needed comparing with experienced operators. This case was also suitable for OCT which showed very good resolution of lesions and stent for PCI guidance.