
CASE20220812_002
Debunking Complex PCI – The Dilemma of Calcified Bifurcation Stenting
By , , , , , , ,
Presenter
Heng Shee Kim
Authors
1, 2, 2, 2, 2, 2, 2, 2
Affiliation
, Malaysia1, , Japan2
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Debunking Complex PCI – The Dilemma of Calcified Bifurcation Stenting
1, 2, 2, 2, 2, 2, 2, 2
, Malaysia1, , Japan2
Clinical Information
Patient initials or Identifier Number
SSH
Relevant Clinical History and Physical Exam
Mr SSH is an 80-year-old ex-smoker with underlying hypertension,an overactive bladder, and a family history of ischemic heart disease,presented with CCS II exertional angina for months. Physical examination wasunremarkable, with a well-controlled blood pressure of 128/70 mmHg and a heartrate of 70 beats per minute.
Relevant Test Results Prior to Catheterization
The electrocardiogram showed no sign of ischemia. The echocardiogramwas normal, with a left ventricular ejection fraction of 58% with no regionalwall motion abnormality. His LDL was 102 mg/dl, eGFR 60 ml/min, and HbA1c of5.7.
He underwent Coronary Computed Tomography Angiography (CCTA),which showed a calcium score of 545 with a high possibility of severe stenosisof the proximal left anterior descending artery (LAD) and modera
He underwent Coronary Computed Tomography Angiography (CCTA),which showed a calcium score of 545 with a high possibility of severe stenosisof the proximal left anterior descending artery (LAD) and modera
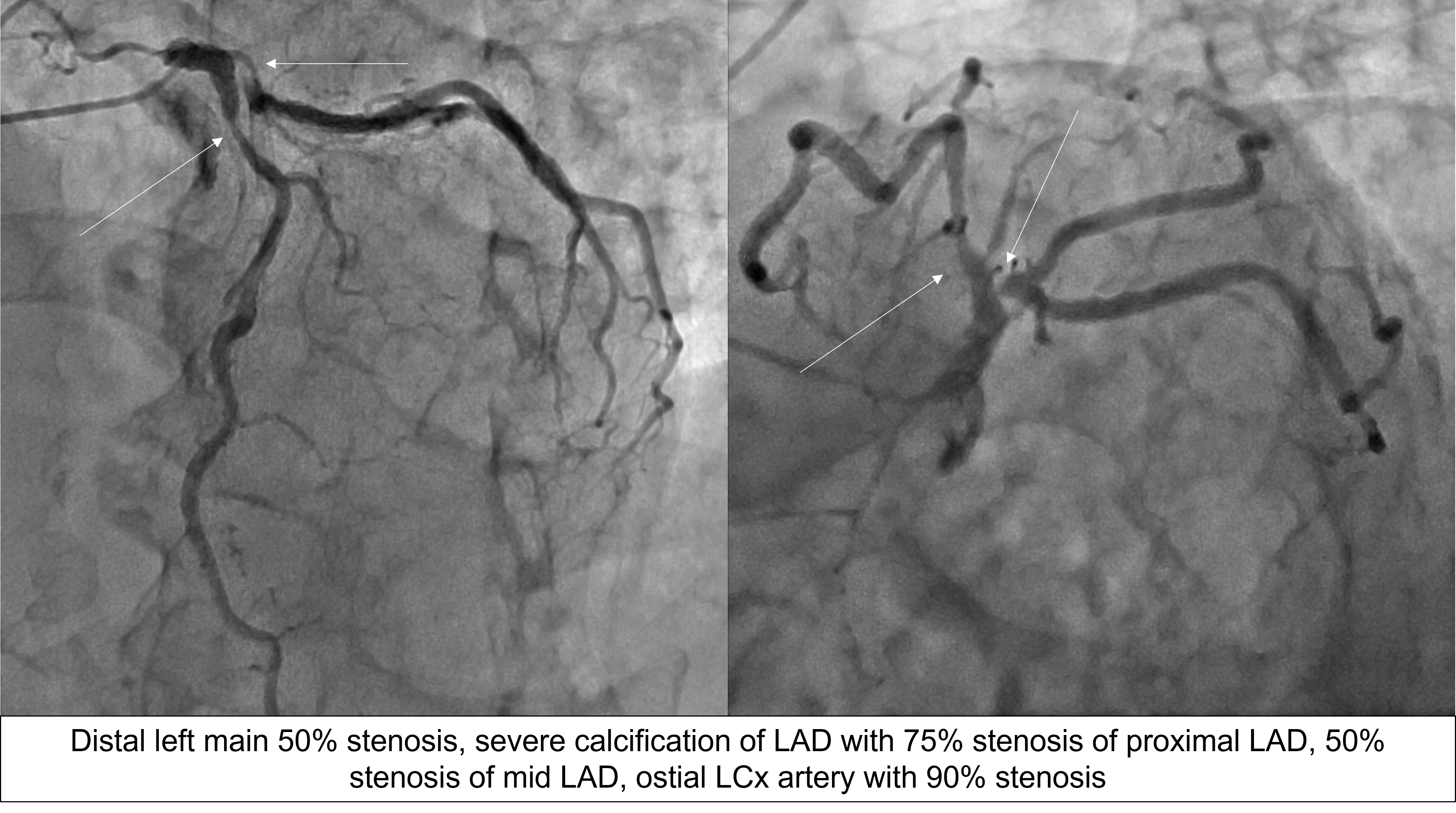
Relevant Catheterization Findings
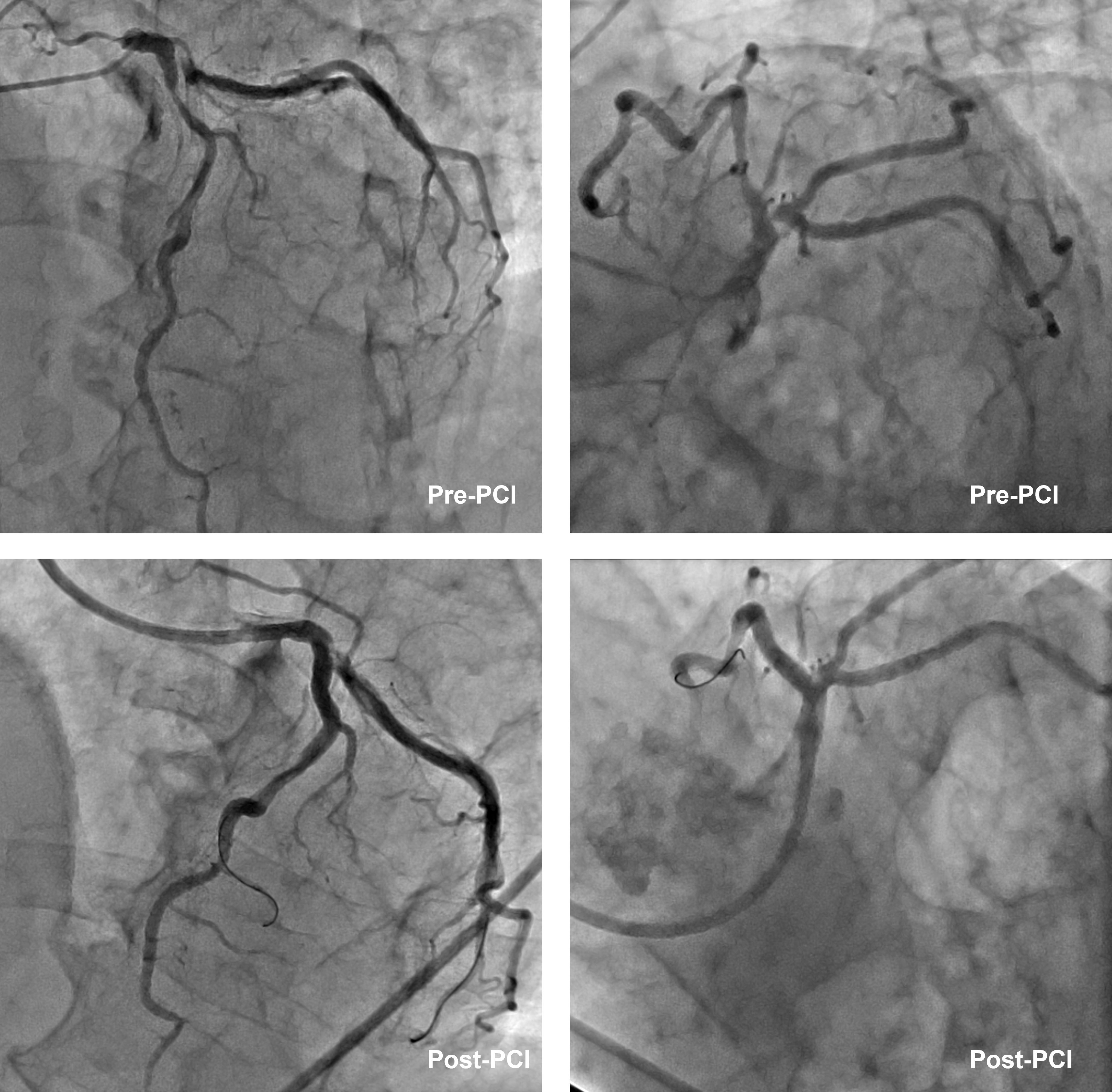
CAG showed distal left main (LM) 50% stenosis, severecalcification of LAD, 75% stenosis of pLAD, 50% stenosis of mLAD,ostial LCx 90% stenosis and mild disease of PDA.LAD FFR was 0.74 with 0.23 step up over thepLAD.
This is a true bifurcation, Medina 1,1,1 lesion with LM involvement. Syntax I score - 30, Syntax II score of PCI vs CABG was 35.9 vs 42.9; with a 4-year mortality of 10.9% vs 18.8%.

 Video A - RCA.mp4
Video A - RCA.mp4
Video B - LCA.mp4
This is a true bifurcation, Medina 1,1,1 lesion with LM involvement. Syntax I score - 30, Syntax II score of PCI vs CABG was 35.9 vs 42.9; with a 4-year mortality of 10.9% vs 18.8%.
After discussion with the patient and family members, he was then planned for PCI to LM, LAD and LCx.
Interventional Management
Procedural Step
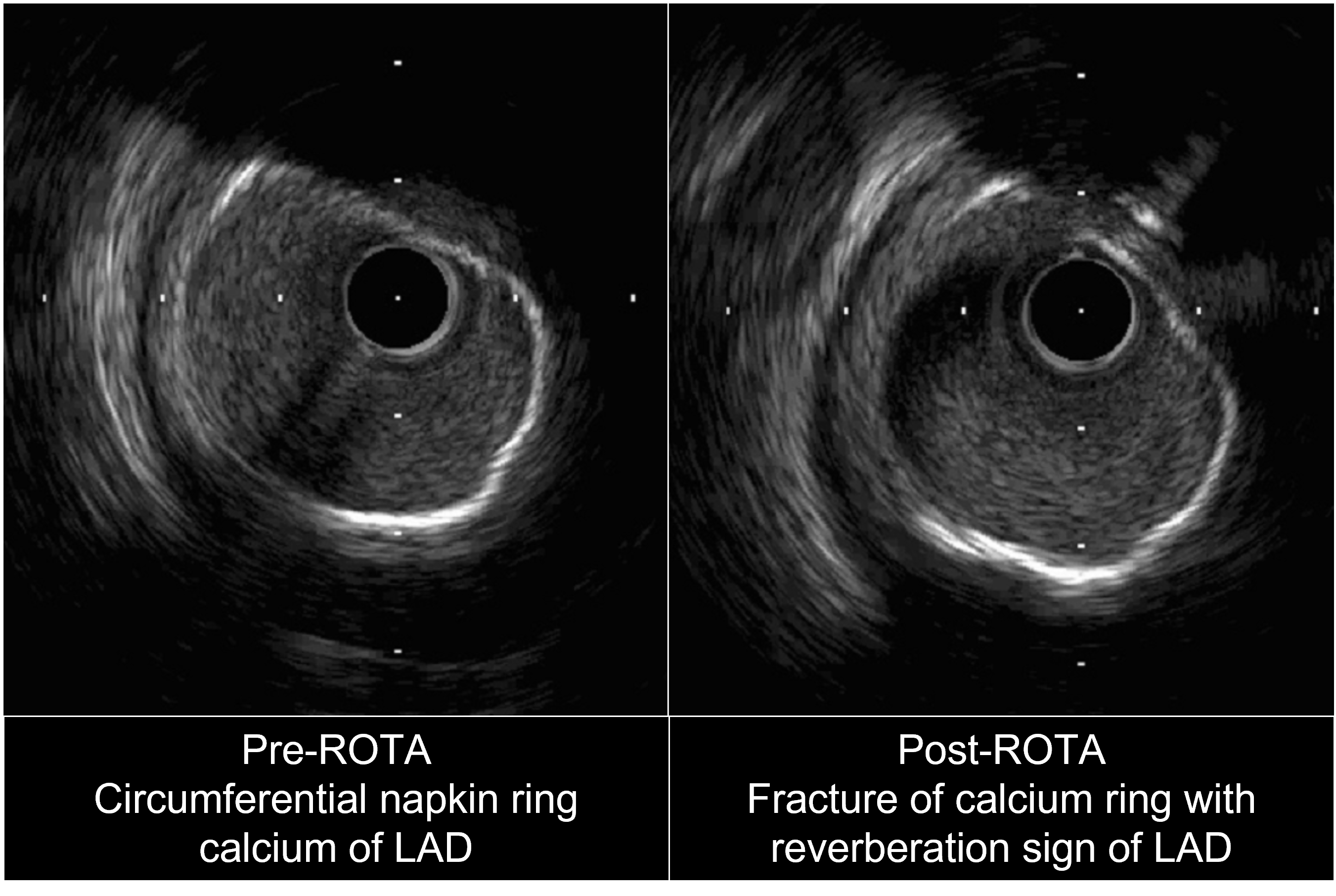
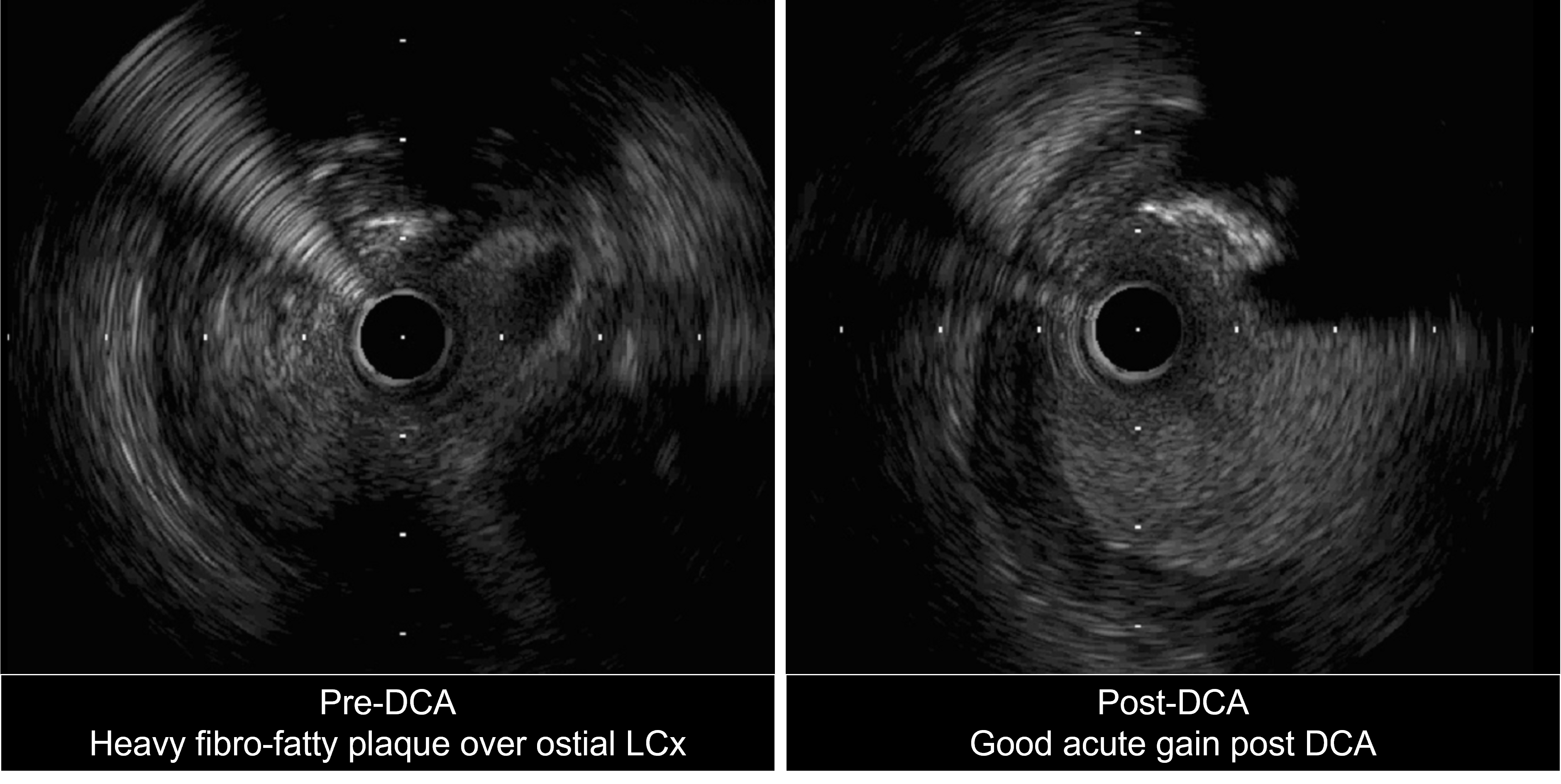
Ostial LCx further prepared with GOODMAN NSE ADVANCE 3.5mm x13mm scoring balloon at 16atm. Distal LM to pLCx treated with SEQUENT PLEASENEO 3.5mm x 15mm DCB at 8atm for 60s. tomLAD prepared with TERUMO RYUREI 3.0mm x 15mm SC balloon followed by NSEADVANCE 3.5mm x 13mm balloon. Then, ostial LAD to mLAD stented with RESOLUTEONYX 3.5mm x 34mm DES under IVUS guidance. Final CAG and IVUS showed good stentapposition and expansion, MLA of 16.81 mm2 for LM, 10.50 mm2 forLCx and 8.9 mm2 for pLAD with no stent edge dissection. Totalprocedure time: 135 minutes; contrast 100ml.
Case Summary
The use of intravascular imaging allows the PCI operator to properlyunderstand the plaque distribution and vessel anatomy, thus, enabling us tochoose the correct debulking tools in a complex calcified bifurcation PCI. Wedemonstrated that the supposedly 2-stent bifurcation PCI can be turned into ahybrid DES-DCB PCI with good angiography and intravascular outcome with the combination use of Rotablation, DCA, and scoring balloon.